Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com
No texting or chat messages, please. Ordinary e-mails are welcome.
|
|
 |
 |
 |
 |
|
verify here. |
Cyberfriends: The help you're looking for is probably here.
This website collects no information. If you e-mail me, neither your e-mail address nor any other information will ever be passed on to any third party, unless required by law.
This page was last modified January 1, 2016.
I have no sponsors and do not host paid advertisements. All external links are provided freely to sites that I believe my visitors will find helpful.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected. No texting or chat messages, please. Ordinary e-mails are welcome.
 I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
 If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |

|
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
 My team:
My team:
pathology.org -- my cyberfriends, great for current news and browsing for the general public
EnjoyPath -- a great resource for everyone, from beginning medical students to pathologists with years of experience
Medmark Pathology -- massive listing of pathology sites
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures
Freely have you received, freely give. -- Matthew 10:8. My site receives an enormous amount of traffic, and I'm still handling dozens of requests for information weekly, all as a public service.
Pathology's modern founder, Rudolf Virchow M.D., left a legacy of realism and social conscience for the discipline. I am a mainstream Christian, a man of science, and a proponent of common sense and common kindness. I am an outspoken enemy of all the make-believe and bunk that interfere with people's health, reasonable freedom, and happiness. I talk and write straight, and without apology.
Throughout these notes, I am speaking only for myself, and not for any employer, organization, or associate.
Special thanks to my friend and colleague, Charles Wheeler M.D., pathologist and former Kansas City mayor. Thanks also to the real Patch Adams M.D., who wrote me encouragement when we were both beginning our unusual medical careers.
If you're a private individual who's enjoyed this site, and want to say, "Thank you, Ed!", then what I'd like best is a contribution to the Episcopalian home for abandoned, neglected, and abused kids in Nevada:
My home page
More of my notes
My medical students
Especially if you're looking for information on a disease with a name that you know, here are a couple of great places for you to go right now and use Medline, which will allow you to find every relevant current scientific publication. You owe it to yourself to learn to use this invaluable internet resource. Not only will you find some information immediately, but you'll have references to journal articles that you can obtain by interlibrary loan, plus the names of the world's foremost experts and their institutions.
Alternative (complementary) medicine has made real progress since my generally-unfavorable 1983 review. If you are interested in complementary medicine, then I would urge you to visit my new Alternative Medicine page. If you are looking for something on complementary medicine, please go first to the American Association of Naturopathic Physicians. And for your enjoyment... here are some of my old pathology exams for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I do not accept donations, though I appreciate those who have offered to help.
During the eighteen years my site has been online, it's proved to be one of the most popular of all internet sites for undergraduate physician and allied-health education. It is so well-known that I'm not worried about borrowers. I never refuse requests from colleagues for permission to adapt or duplicate it for their own courses... and many do. So, fellow-teachers, help yourselves. Don't sell it for a profit, don't use it for a bad purpose, and at some time in your course, mention me as author and William Carey as my institution. Drop me a note about your successes. And special thanks to everyone who's helped and encouraged me, and especially the people at William Carey for making it still possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it, here or elsewhere. Health and friendship!

![]()
![]()
We have two ends with a common link;
With one we sit, with one we think.
Success depends on which we use;
Heads we win, tails we lose!
--Author unknown
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
![]() KCUMB Students
KCUMB Students
"Big Robbins" -- GI Tract
Lectures follow Textbook
QUIZBANK
GI tract (all)
 Consider this mastery material.
Consider this mastery material.
Be sure you can use the following terms correctly, and tell how and where they apply to the gut.
achalasia
atresia
diverticulum
erosion
fistula
hematemesis
hematochezia
hernia
melena
polyp
pseudo-diverticulum
reflux
stenosis
tenesmus
ulcer
Be sure you can recognize each of the kinds of lesions presented on the videodisc!
INTRODUCTION
|
|
Disease of the gut troubles most people at some time during their lives, and claims the lives of many people.
This easy unit focuses on problems with the alimentary canal. Conceptually, the material presents no serious problems. Some of the "why"'s are only now being clarified, and several common problems have complex causes. The human gut withstands considerable abuse. For a review of the many injuries to which the gastroduodenal mucosa is subject, see J. Clin. Gastroent. 13(S1): S1, 1991.
A few terms for review now:
POLYP: Any bump on the gut that sticks up above the inner surface into the lumen.
HERNIA: Presence of a portion of an organ in a body space where it doesn't belong. INCARCERATED HERNIA: One that can't be REDUCED, i.e., put back in its proper place. STRANGULATED HERNIA: Where venous drainage is compromised and infarction is imminent / present.
EROSION: A portion of the epithelium of a mucosal surface has been lost due to necrosis, but there has been little or no loss of the underlying connective tissue. In the stomach, as the term is generally used, there may be loss of some connective tissue but sparing the muscularis mucosae.
ULCER: A portion of the epithelium AND some of the connective tissue has been lost due to necrosis. In the stomach, an "ulcer" is typically diagnosed only if the muscularis mucosae is lost.
DIVERTICULUM: An outpouching of all the layers of the wall of a hollow organ. PSEUDO-DIVERTICULUM: Outpouching of mucosa through a defect in the muscularis propria.
PARACRINE / ENDOCRINE CELLS ("Kulchitsky cells", "enterochromaffin", "enteroendocrine", "neurosecretory", "argentaffin / argyrophil", formerly "APUD" cells) are found individually all along the gut, and various ones produce various peptide hormones of known and unknown significance. (You met these in the lung when we studied oat cell carcinoma and bronchial carcinoid.)
In the GI tract in particular, "atypia" and "dysplasia" are more-or-less interchangeable terms.
Although lymphocytes are numerous in the lamina propria, they are never normal in any portion of the epithelium itself.
The common cancers of the GI tract are carcinomas. Often the first physical finding is Virchow's sentinel lymph node, where the thoracic duct joins the left internal jugular vein.
For the basics of the GI viruses, click here.
Remember that blood that stays in the stomach for a while before being vomited / removed by tube will look like "coffee grounds" ("acid hematin"). Upper GI bleeding that produces diarrhea will produce melena (black tarry stools with an odor you'll come to know well), while bleeding from the hindgut will usually be bright red (hematochezia).
ESOPHAGUS
|
|
|
The "gullet" begins at the cricopharyngeus (the short "upper esophageal sphincter" starts here) and ends at the diaphragmatic hiatus or thereabouts ("lower esophageal sphincter"). Solid food may hang up at either site, or where the esophagus passes behind the left main-stem bronchus or between enlarged hilar nodes. Neither sphincter is fool-proof (or even anatomic). Considerable coordination is required for a proper swallow (the big word for "swallowing" is "deglutition"). Most of the time, the esophagus performs its simple but important task well.
You remember that the upper esophagus (i.e., the first inch or so) has mostly skeletal muscle (and is thus subject to diseases of nerve and skeletal muscle), the middle esophagus (i.e., maybe another inch) has both skeletal and smooth muscle, and the distal esophagus (i.e., most of the esophagus) has mostly smooth muscle. Unlike most of the rest of the gut, the esophagus has no serosa to help limit the spread of rips or cancers.
Problems with the esophagus manifest as difficulty and/or pain on swallowing, and/or problems with regurgitation.
BIRTH DEFECTS of the esophagus are relatively common.
AGENESIS of some or all of the esophagus is uncommon. ATRESIA of the esophagus, as elsewhere, is failure of a normally-hollow organ to develop its lumen. An atretic esophagus is represented, over part or all of its length, by a fibromuscular cord without a lumen. Less severely, portions of the esophagus may be congenitally STENOTIC (i.e., too narrow).
{20073} esophageal atresia, from behind. Lungs at the sides, stomach at the bottom
TRACHEO-ESOPHAGEAL FISTULAS of several varieties are common neonatal surgical problems. The proximal esophagus may enter the trachea or bronchus, producing coughing upon feeding (* original movie of M*A*S*H). The proximal esophagus may end blindly and the distal esophagus arise from a large airway, preventing feeding and causing the stomach to fill with air (the most common version). Or there may simply be a window between the two organs.
THROAT PROBLEMS: A little bit higher than the real esophagus, but worth mentioning here:
GLOBUS PHARYNGEUS ("globus syndrome", "globus hystericus"), a "lump in the throat", is spasm of the back of the throat and perhaps the upper esophagus. It creates the feeling of a mass in the hypopharynx. Sometimes the cause is organic (i.e., a reflex from something wrong nearby, perhaps reflux from the esophagus spilling into the larynx; or a thyorid nodule that was missed -- J. Laryngol. Otol. 121: 242, 2007); often it's psychosomatic. Psychiatrists attribute it to "swallowed tears", and the cure is to cry. (Despite its banal nature, the sensation of a mass may frighten a patient. "Spontaneous cures of non-biopsy-proven throat cancer" sound like globus.)
ZENKER'S "PULSION" DIVERTICULUM: Adjacent to the cricopharyngeus muscle. A hiding-place for last week's spaghetti and last month's pills (so THAT'S why they didn't work....) The smell alone may create a serious social problem.
An EPIPHRENIC DIVERTICULUM, also of mysterious origin, occurs just above the diaphragm. It can harbor large amounts of fluid that are disgorged back to the mouth shortly after the patient goes to bed.
ACHALASIA means "failure of a sphincter to relax when it should". Usually, this means the lower esophageal sphincter. Update Lancet 383: 83, 2014; JAMA 313: 1841, 2015.
In the U.S., the problem is usually idiopathic failure of the lower sphincter to relax. The etiology is just now becoming clarified; the cause is usually inflammation of the myenteric plexus (Am. J. Surg. Path. 24: 1153, 2000; Histopathology 35: 445, 1999; Gastroenterology 111: 648, 1996), with eventual nerve damage, but nobody knows why this happens ("aberrant immune response following a viral infection"). In other cases, the ganglion cells are simply lost instead; no one knows why.
The esophagus remains filled with food. The patient (typically a young adult) will notice regurgitation and bad breath. The situation may become really nasty as more and more food accumulates in a mega-esophagus. Fortunately, most patients are cured by a single endoscopic dilatation of the sphincter; there's also "botox", or laparoscopic myotomy and partial fundoplication for the hard cases (Am. J. Surg. 181: 471, 2001.)
Untreated, achalasia is a life-threatening problem (carcinoma, aspiration pneumonia). The Heller myotomy and balloon pneumatic dilatation are both standard treatments and seem to work equally well.
* Pseudo-achalasia usually results from cancer obliterating the myenteric plexus (Am. J. Surg. Path. 26: 784, 2002).
You remember that Chagas' disease (T. cruzi) is an important cause of mega-esophagus where it is endemic.
GLYCOGEN PLAQUES are acanthotic (i.e., thick spiny layer) epithelium with extra glycogen. The most common lesion of the esophagus, and of no consequence. You'll see it frequently if you do endoscopies.
* Occasionally, endoscopists see a very dark-pigmented esophagus without any other pathology. This is esophageal melanocytosis (Arch. Path. Lab. Med. 130: 552, 2006); its significance remains unknown.
WEBS are contracted, localized fibrous scars that form little shelves ("ledges") that may obstruct the lumen.
* No one knows quite what to make of a supposed association between upper esophageal webs, iron deficiency anemia, and a risk for squamous cell carcinoma in the proximal esophagus. Whether or not this really exists, it's called "Plummer-Vinson syndrome". Current thinking is that somehow iron deficiency causes the webs to form just beyond the cricoid (Am. J. Gastro. 97: 190, 2002).
SCHATZKI'S RING (B-RING) is a washer-shaped partially-obstructing fibrous mucosal ring at the squamo-columnar junction just above the gastroesophageal junction. The upper surface is covered with squamous epithelium, and the lower surface with columnar. It is a radiologist's delight and may turn up on imaging / endoscopy in any adult; long a mystery, cases that occur in the absence of reflux may be due to pill enlodgement (Am. J. Surg. 158: 563, 1989). A-RING is muscular, usually about 2 cm the gastro-esophageal junction.
A big chunk of solid food (i.e., poorly-chewed beef) may hang up on a web or ring. In bad cases, softer food may have trouble negotiating the obstruction.
{09433} Schatzki ring
{09434} Schatzki ring
{09435} web
HIATUS HERNIA is said to be present whenever a portion of the stomach pooches up through the diaphragmatic hiatus. Said to be present in up to 10% of adults (typically the overweight), they are most often sub-clinical.
SLIDING HIATUS HERNIA (the usual kind) is present when a short (congenital, fibrous scarring from years of reflux, diaphragm pulled low by obesity) pulls the proximal stomach into the chest. As the esophagus contracts during swallowing, radiologists watch the stomach slide further up through the diaphragm. As with "reflux esophagitis", the distal esophagus is likely to become inflamed and damaged as a result of exposure to pepsin and acid. It's very common and only 5% of people who have a sliding hiatus hernia are symptomatic from it.
PARA-ESOPHAGEAL ("ROLLING") HIATUS HERNIA (the less common kind) is present when a portion of the stomach rolls up through the diaphragm alongside an esophagus of normal length. This may be asymptomatic, but the herniated portion of stomach may become strangulated.
Future pathologists: Don't expect to see either type of hernia (or, for that matter, a Schatzki's ring, or an intestinal hernia) after death, when the muscles of the body relax / go into rigor mortis.
TRACTION DIVERTICULUM results from scar
contraction in the mediastinum (i.e., TB![]() ). They are uncommon.
). They are uncommon.
* APHTHOUS ULCERS, the familiar painful white "canker sores" that most people have experienced on the oral mucosa, may be a serious problem in the esophagus for people with HIV infection. No one knows why. Thalidomide for this problem: J. Inf. Dis. 180: 61, 1999.
GASTROESOPHAGEAL REFLUX DISEASE (GERD, formerly, "peptic esophagitis") is THE common esophagal problem, the result of an incompetent lower esophageal sphincter. Review Lancet 381: 1933, 2013.
The sphincter is inflamed, scars, and becomes further damaged. The epithelium keeps getting digested and regrowing, with much more opportunity to select for mutated cells. Pathophysiology Am. J. Med. Sci. 326, 274, 2003.
Update for clinicians: JAMA 287: 1972 & 1982, 2002. If the patient with "GERD" symptoms has no erosions on endoscopy, it's "NERD" (non-erosive reflux disease". Esophagitis update for pathologists: Arch. Path. Lab. Med. 133: 1087, 2009. Around 20% of people in the US have "heartburn" in a given week; for around 40% of people with heartburn it is a mere nuisance. Others are not so fortunate. The worst cases get GI bleeding (especially if there's portal hypertension this can kill a person) and/or fibrosis / stricture. The correlation between clinical symptoms and endoscopy is remarkably poor. Only about half of the patients with severe "GERD" on endoscopy even have heartburn (Dig. Dis. Sci. 48: 2237, 2003.)
* Like most other diseases of children, pediatric GERD gets blamed on cow's milk. Since the disease also occurs in children who do not drink cow's milk, it cannot be the sole cause. And since the only test is an elimination diet and response to challenge (still true Arch. Dis. Child. 92: 902, 2007), and since strongly-held emotionally-based beliefs are involved, getting at the truth will be difficult. A pop claim that eosinophils in the upper GI mucosa identified the subset of cases caused by milk allergy failed a scientific study miserably (J. Clin. Path. 59: 89, 2006).
* A few folks with GERD symptoms (even "chest pain") but normal endoscopy may have "hypersensitive esophagus" and response to a low-dose SSRI. Ask a gastroenterologist.
The cause of common "reflux" remains obscure. Mechanical problems (including overweight and
sliding hiatus hernia) must contribute, and the problem is more severe if there's "excess stomach acid
/ pepsin / bile" or the gastric contents stays for some reason within the esophagus. Other things that
irritate the esophagus (swallowing spicy food, alcohol, very hot
beverages, and/or tobacco juice) will not help either. Pregnancy, benzodiazepines, intubation, and
tobacco use are all implicated as well. Lying flat makes matters worse (tip: try propping the head of
the bed up on cinder blocks --- this may even save your ventilator and nursing-home patients
much grief).
The diagnosis of GERD is made clinically on endoscopy
(Dig. Dis. Sci. 45: 217, 2000),
but pathology may be obtained for confirmation.
* Here's
the new scoring system for reflux (Dig. Dis. Sci. 56: 2656, 2011):
HOW TO SCORE IT: Future pathologists: Be sure you've got that specimen properly oriented, and consider asking the
clinician to send it up on cardboard;
Why the thickness of the basal cell layer? In reflux, the surface cells get digested and the basal cells
are multiplying overtime to replace them.
Just to complicate things, some pathologists say that
"carditis" -- lots of neutrophils in the mucosa of the cardia of the stomach,
but not the rest of the stomach -- may be the best marker.
![]() Peptic esophagitis ulcers
Peptic esophagitis ulcers
WebPath Photo
One "1" is normal
Two or three "1"'s or a "1" and a "2" is mild
Four "1"'s or two "2"'s is severe.
{19451} histopathology of reflux (basal cell hyperplasia)
If replacement of the normal squamous epithelium by a columnar epithelium has occurred, you may have a BARRETT'S ESOPHAGUS. It's supposedly always caused by reflux. Even one goblet cell with acid mucin makes it a Barrett's; some (England, Japan) say any columnar change is Barrett's while others (USA) require some intestinal metaplasia (in the USA, we call replacement of the distal esophagus by gastric-type mucosa "gastric metaplasia"). All about Barrett's: Gastroenterology 122: 1569, 2002; NEJM 346: 836, 2002; Med. Clin. N.A. 86: 1423, 2002; Arch. Path. Lab. Med. 132: 1577, 2008; Arch. Path. Lab. Med. 134: 1589, 2010; Arch. Path. Lab. Med. 135: 1249, 2011; Lancet 373: 850, 2009; mega-position-paper Gastroenterology 138: 854, 2010; a pathologist writes about the difficulties in the current systems (Arch. Path. Lab. Med. 134: 1479, 2010).
It's common to have a bit of columnar epithelium above the diaphragm, and some folks require 3 cm of "Barrett's" in the tubular esophagus before they're willing to call it. As noted, some definitions of Barrett's require goblet cells ("and one is sufficient to make the diagnosis"), while others note that goblet cells actually seem to regress as cancer develops. For the truly hardcore, the non-goblet cells are both absorptive and secretory. It is not clear whether goblet cells are required for progression to cancer.
* Future pathologists -- "Blue mucin" in a columnar cell is a variant that's not a goblet cell.
Pathologists distinguish Barrett's from common (perhaps inflamed) gastric cardia by looking for... (Am. J. Surg. Path. 31: 1733, 2007):
There are at least 2 million "Barrett's" patients in the U.S; with a 3:1 male predominance (no one knows why). In Sweden, 1.6% of the population is affected, with alcohol and tobacco being risk factors (Gastroent. 129: 1825, 2005); by contrast, neither smoking nor drinking seems to be a risk factor in Texas (Dig. Dis. Sci. 59: 108, 2014).
As you'd expect ("Nowell's law triumphant"), finding a Barrett's esophagus means there's been some hits on the genome, and the genetically damaged cells have had a chance to overgrow the area because of repeated healing from reflux. This is a fertile breeding ground for adenocarcinoma of the esophagus.
* The molecular biology of transformation to cancer is now well-established: Dig. Dis. Sci. 56: 3405, 2011; a few germline mutations are common both in patients with Barrett's esophagus and esophageal adenocarcinoma (JAMA 306: 410, 2011). Loss of p16INK4a by methylation seems to transform Barrett's to cancer (Virch. Arch. 445: 135, 2004).
* Anti-reflux therapy may be helpful, but don't count on it to reverse the process. This includes the new, popular procedure of laparoscopic fundoplication (Ann. Thor. Surg. 77: 393, 2004).
In today's cost-conscious era, it seems reasonable to screen adults who complain of heartburn once for Barrett's, with follow-up if and only if there is dysplasia (numbers Ann. Int. Med. 138: 176, 2003; further support for this common-sense idea NEJM 365: 1375, 2011).
More on mutations in Barrett's: Arch. Surg. 132: 728, 1997. Deciding on therapy (lasers / photodynamic therapy -- dysplastic cells soak up and hold injected porphyrins unlike normal cells --, electrocoagulation, mechanically removing the mucosa, surgery) based on how bad the dysplasia is: Br. J. Surg. 84: 760, 1997, Am. J. Med. 111 S 8A: 147A, 2001; lasers see Gut 51: 776, 2002. Today, radiofrequency ablation is the mainstay of treatment, is less likely to result in complications such as stenosis compared to endoscopic resection, and seems to last at least 3 years in the vast majority of patients (Gastroenterology 141: 460, 2011; Gastroenterology 145: 87 & 96, 2013). Today, eradication by radiofrequency ablation is the norm for high-grade dysplasia, an option for low-grade dysplasia, and not recommended for no-dysplasia (JAMA 310: 627, 2013).
Future pathologists: You'll look at dysplasias from Barrett's biopsies frequently, and there are likely to be further refinements that will help you let the surgeons know when to operate (laser, scrape, etc). All Barrett's have some hyperchromasia of the nuclei in the lower portions of the glands. Low-grade dysplasia (0.25% / year chance of turning to cancer) features loss of mucus production, stratified nuclei in the crypts, and elongated hyperchromatic nuclei in parallel -- cigar nuclei. High-grade dysplasia (6% chance / year of turning to cancer) features loss of nuclear polarity (i.e., they no longer line up with their neighbors -- this is key), stratification on the surface, branching glands, and/or cribriform stuff in the crypts. Be careful about calling "severe dysplasia" if there is inflammation; it might be better to treat the reflux and repeat the biopsy. One major criterion that says "operate" is loss of the basal orientation of the nuclei, i.e., this is more than just the kind of atypia that one finds in an adenomatous polyp. Grading updates: J. Clin. Path. 55: 910, 2002; J. Clin. Path. 59: 1029, 2006. Biomarkers Mayo Clin. Proc. 76: 438, 2001. Does screening really save enough lives to be worthwhile? It's still a tough call (Am. J. Gastro. 98: 1931, 2003; Gastroenterology 127: 310, 2004 from KU). Treatment update: JAMA 310: 627, 2013.
* HCA, an immunostain to help spot the aggressive dysplasias: Am. J. Clin. Path. 122: 747, 2004. Update: A panel of cancer markers all tend to turn positive as the dysplasia develops and progresses; beta-Catenin/CNTTB1 staining means at least low-grade dysplasia rather than metaplasia (though many remain negative), and cyclin D1 and p53 indicate an aggressive dysplasia regardless of histology (Am. J. Clin. Path. 130: 745, 2008; Gut 62: 1676, 2013).
{15428} Barrett's esophagus (note tan columnar, rather than white squamous, mucosa)
{15429} Barrett's esophagus
{15427} acute reflux esophagitis (one heck of a case of heartburn;
stomach is on the left)
* Worth mentioning only because people get excited: Maybe one person in four who gets an esophageal-gastric junction biopsy has a few glands that look like pancreatic acini ("pancreatic acinar metaplasia"). It means nothing. Since it's more common in older folks, it probably really is a metaplasia rather than a birth variant.
Reflux leads to fibrosis (scarring, shortening, perhaps narrowing) of the esophagus, difficulty on swallowing ("DYSPHAGIA"), pain in swallowing ("ODYNOPHAGIA"), retrosternal pain ("heartburn") and/or slow GI bleeding leading to iron-deficiency. In severe cases, massive GI bleeding (hematemesis, melena) can occur.
Other noteworthy causes of ESOPHAGITIS include candida![]() (think of this whenever you see a lot of neutrophils),
CMV
(think of this whenever you see a lot of neutrophils),
CMV![]() ,
herpes
,
herpes![]() ,
radiation, generalized
diseases of stratified squamous epithelium (* pemphigus, other),
pill esophagitis (lots of neutrophils, epithelium mostly gone, no candida), or keeping a stomach tube down for
more than a few minutes. All the above can give some nasty ulcers.
,
radiation, generalized
diseases of stratified squamous epithelium (* pemphigus, other),
pill esophagitis (lots of neutrophils, epithelium mostly gone, no candida), or keeping a stomach tube down for
more than a few minutes. All the above can give some nasty ulcers.
|
|
You also remember the esophageal changes ("rubber hose") in scleroderma (review for pathologists Gut 55: 1697, 2006; circular layer gets it worst) and the similar graft-vs.-host disease.
|
|
{11096} candida esophagitis (scrapes off, unlike glycogen acanthosis)
{11099} candida esophagitis
{49128} candida esophagitis
|
|
{19449} herpes, histology
{25910} herpes, pap smear
* Future pathologists: Herpes![]() of the esophagus is often relatively devoid of good herpes-inclusion
of the esophagus is often relatively devoid of good herpes-inclusion![]() cells. Look instead for clusters of macrophages (Hum. Path. 22: 541, 1991).
cells. Look instead for clusters of macrophages (Hum. Path. 22: 541, 1991).
Drinking lye (Drano, etc., an extremely painful and unreliable method for would-be suicides) or some other caustic substance leads to corrosive esophagitis, strictures, etc., etc. Dig. Dis. Sci. 54: 980, 2009.
* "Black esophagus" ("necrotizing esophagitis") is probably due to necrosis from vascular disease / low output; stomach obstruction may contribute as well by raising pressures here; it's a rare finding at autopsy Am. J. For. Med. Path. 34: 16, 2013. The necrosis and acute inflammatory response show no distinctive features.
{11772} lye burn of stomach
{15554} lye burn of stomach
EOSINOPHILIC ESOPHAGITIS, mostly seen in youngsters but not-unknown in adults, features clusters of eosinophils in the epithelium and underlying connective tissue. It's only been known since the 1990's.
It's supposed to be the second-most-common finding on endoscopy, and regrettably can't always be told from GERD by the pathologist. Patients may recognize the food or inhalant that makes it worse. Patients have dysphagia out-of-proportion to the endoscopic findings, do not respond to anti-acid treatments, sometimes progress to impaction of food at the gastroesopinageal junction, and/or fibrosis of the esophagus which is serious. A trial of an elimination diet can be very helpful. There may or may not be concurrent asthma. See Am. J. Clin. Path. 131: 788, 2009; Arch. Path. Lab. Med. 131: 777, 2007; Arch. Path. Lab. Med. 134: 815, 2010; "mild disease in adults is under-recognized: Dig. Dis. Sci. 56: 1981, 2011; J. Clin. Path. 66: 399, 2013. It's often not possible to be certain just on the histopathology whether you're looking at reflux or "EE"; clinical correlation is recommended (Arch. Otol. 135: 95, 2009). The etiology remains unknown; consider a consultation with an allergist, and treating it as an allergy (eliminating allergens, a bit of fluticasone -- take puffs and swallow) reverses both eosinophilia and fibrosis Dig. Dis. Sci. 56: 97, 2011.
* Mayo's suggests a trial of an elimination diet for this, and reminds readers this can be tried for many other things: Mayo Clin. Proc. 82: 1541, 2007. Elimination diet (or at least elimination of food allergens) and topical fluticasone or budesonide on the esophagus are now standard (Gastroenterology 139: 418 & 1526.e1, 2010; Dig. Dis. Sci. 56: 92, 2011).
PILL ESOPHAGITIS is thankfully uncommon today. The worst was the old potassium chloride tablets for patients on potassium-wasting diuretics.
BISPHOSPHONATE ESOPHAGITIS features nonspecific changes (inflammation, ulcers, erosions) but can be severe.
PERFORATED ESOPHAGUS can result from swallowing the wrong thing. Chicken bones are infamous (AJFMP 19: 166, 1998) -- these can pierce the heart or cause other dreadful problems.
LACERATED ESOPHAGUS usually results from heavy-duty vomiting during which the esophagus fails to relax (alcohol abuse, pregnancy, post-anesthesia; MALLORY-WEISS SYNDROME). Endoscopists and pathologists see little longitudinal tears, usually in the distal esophagus. They are a problem only if bleeding is massive, or if the esophagus actually ruptures (BOERHAAVE'S SYNDROME; at these sites of rupture, the muscularis mucosae was apparently absent: Am. J. Surg. 158: 420, 1989).
{15420} lacerated esophagus
ESOPHAGEAL VARICES are dilatations of the esophago-gastric venous plexus. These result from portal vein hypertension from any cause, as the blood from the stomach and intestines seeks the low-pressure pathway back to the heart.
You won't know varices are there until they bleed. And they bleed massively when their attenuated overlying mucosa is rubbed away, or they just pop from pressure. This is the fast way out of life for many problem drinkers.
{38629} varices, gross
{38632} varices, gross
{15419} esophageal varix, histology
{24406} varices, histology
{40724} varix with clot, histology
Portal hypertension patients will also commonly exhibit hemorrhoids and dilated veins around the umbilicus ("caput medusae", why?) Remember that portal hypertension will greatly accelerate GI bleeding from non-variceal causes (gastritis, peptic esophagitis, ulcer, Mallory-Weiss) as well.
Learn now: THE CAUSES OF PORTAL HYPERTENSION....
BENIGN TUMORS OF THE ESOPHAGUS: Banal, and relatively uncommon. For example, fibrovascular hamartomas: AJR 166: 781, 1996.
CARCINOMA OF THE ESOPHAGUS strikes around 8000 people each years and kills most of them.
|
|
|
ESOPHAGEAL CARCINOMA now affects over 450,000 people worldwide each year, with the numbers rapidly increasing. Both squamous cell carcinoma and adenocarcinoma (especially in the developed nations) are very common nowadays (big review Lancet 381: 400, 2013).
SQUAMOUS CELL CARCINOMA has historically been the most common esophageal cancer in the United States, but is becoming less common.
Most patients are males (more than 4:1), black men are at higher risk than others (still true, mix of genetics and environment Dig. Dis. Sci. 56: 3577, 2011), and in the U.S., the large majority are both smokers (cigarets, cigars) and drinkers.
Old lye strictures are also frequent sites for esophageal cancer, as is the Chagas-disease ridden mega-esophagus (Digestion 47: 138, 1990).
The epidemic of highly-aggressive squamous cell carcinoma in Mainland China (Cancer 73: 2027, 1994;
Cancer 74: 573, 1994) has been attributed to
aspergillus![]() fungus contamination, nitrosamines,
vitamin deficiency, zinc deficiency, molybdenum deficiency, ethnic teas, and ethnic delicacies that
are pickled (i.e., rendered rich in certain fungi).
It's common knowledge that much of China remians selenium deficient because
of ongoing government indifference (Am. J. Clin. Nutr. 79: 80, 2004;
Cancer 106: 2345, 2006).
China's scientists are forced to remain silent -- a frankly funny paper claimed that people
in the area had genetic susceptibility to p53 mutations (!! Cancer 101: 834, 2004).
Mongolia has the world's highest incidence.
fungus contamination, nitrosamines,
vitamin deficiency, zinc deficiency, molybdenum deficiency, ethnic teas, and ethnic delicacies that
are pickled (i.e., rendered rich in certain fungi).
It's common knowledge that much of China remians selenium deficient because
of ongoing government indifference (Am. J. Clin. Nutr. 79: 80, 2004;
Cancer 106: 2345, 2006).
China's scientists are forced to remain silent -- a frankly funny paper claimed that people
in the area had genetic susceptibility to p53 mutations (!! Cancer 101: 834, 2004).
Mongolia has the world's highest incidence.
* The South Carolina lowlands have a great excess of squamous cell carcinoma of the esophagus, and these cancers have a distinctively high rate of p53 mutations, suggesting some chemical in the environment (J. Thor. Card. Surg. 108: 148, 1994). Is it their moonshine? Still a mystery: South. Med. 95: 900, 2002. In West Kenya, it is a common disease of teens and young adults (Lancet 360: 462, 2002).
Any portion of the esophagus can be involved; the middle third is slightly more common than the others.
Like most squamous cell carcinomas, esophageal cancer arises in squamous dysplasia (update Gut 54: 187, 2005), is often multifocal (Cancer 73: 2687, 1994), grows as a fungating lesion (less often, just an ulcer), and produces symptoms (dysphagia, food "sticking") only late. Because of its location, the later stages of this disease are particularly cruel.
* Leave the distinctions among common squamous carcinoma and its uncommon verrucous, spindle-cell, basaloid (cells with very scanty cytoplasm but that do have squamous markers on special stains), and adenosquamous forms to us.
* Biomarkers: Surgery 127: 552, 2000.
* HPV is present in perhaps a quarter of esophageal cancers; no one knows what this means (J. Clin. Path. 55: 721, 2002).
* Honesty or the impact of managed care? The surgeons tell it like it is: radiation and chemotherapy for cancer of the esophagus have little or no impact beyond making life more miserable for these patients (Arch. Surg. 133: 722, 1998).
{15423} carcinoma of the esophagus, exophytic growth
{15421} carcinoma of the esophagus, growing as ulcer
{15422} carcinoma of the esophagus, annular growth
{15424} squamous carcinoma of the esophagus, histology
{15552} carcinoma of esophagus invaded aorta
{19345} yet another squamous cell carcinoma of the esophagus (x-ray)
{26876} and another
{42231} and still another
ADENOCARCINOMA (CA 63: 232, Jul-Aug 2013) is now almost as common as squamous cell carcinoma in the United States, and is increasing tremendously in frequency. (Worldwide, the vast majority of esophageal cancers are still squamous.) It usually has the "intestinal histologic subtype" seen in stomach cancers (see below). It arises most often in a Barrett's esophagus. Again, the male predominance is marked (more than 6:1, no one knows why); this is related (as in gastric intestinal cancers) to the fact that women develop them much later in life, usually long after menopause (Gut 58: 16, 2009) -- i.e., it's a hormonal effect. As you'd expect, symptomatic reflux is a strong risk factor (NEJM 340: 825, 1999). Tobacco and obesity are supposed to be risk factors, alcohol consumption is not (confirmed Gut 60: 1029, 2011); once Barrett's is detected, no known risk factor contributes to progression (Dig. Dis. Sci. 53: 1175, 2008). The longer the Barrett's region (Gut 33: 1155, 1992), the higher the risk, and smoking also increases risk: Cancer 72: 1155, 1993 (big study).
The increasing incidence may be due to pathologists no longer calling these stomach cancer, and almost certainly as well to the increasing prevalence of obesity and reflux.
Prognosis depends on both grade and stage at the time of resection. Signet-ring cells especially impart a more severe prognosis (Mayo Clin. Proc. 85: 1080, 2010; Cancer 119: 3156, 2013; Ann. Thor. Surg. 96: 1927, 2013; very early cancer may be an exception Surgery 154: 1093, 2013).
Future pathologists: TTF-1 and napsin A -- "lung markers" -- are often positive in primary esophageal adenocarcinoma (Arch. Path. Lab. Med. 137: 1094, 2013 -- advises some more specific stains when you must make the distinction).
![]() Barrett's esophagus with cancer
Barrett's esophagus with cancer
Joel K. Greenson MD
U. of Michigan
Other tumors of the esophagus are banal (little leiomyomas) or vicious rare lesions (sarcomas; melanomas, Arch. Path. Lab. Med. 132: 1623 & 1675, 2008, oat-cell Ann. Thorac. Surg. 91: 373, 2011).
{49132} leiomyoma, gross
|
{11889} stomach with biscuit
|
 "Sometimes nothing can be a pretty cool hand." |
|
|
|
Most stomach problems start with the mucosa. Review of the healthy mucosa:
Surface, pits ("crypts" / "foveolae", confusingly named because they are on the surface) in all areas... Tall surface mucous cells (make "neutral mucus")
Deep in pits, all areas... Neck cells (reserve cells for both above and below; "the proliferative zone")
Cardiac glands... More neck-type cells
Gastric glands... Parietal cells (eosinophilic, packed with mitochondria; make acid and intrinsic factor); Chief cells (pale, granular); ECL ("enterochromaffin-like") cells (histamine-makers, also probably make other hormones). The gastric gland layer is about 4x as thick as the gastric pit layer.
Pyloric glands... Neck-type cells; G-cells (gastrin producers). The pyloric gland layer is about equally thick as the pit layer.
* In 1999, Lancet 354: 134, 1999 published a short report on biotech-enhanced potatoes thickening the mucosa of the stomach and elongating the crypts of rats to which they were fed. A small-sample study with a conclusion that didn't make sense... and the small differences could easily be explained by differences in the angles produced by hand-cutting and hand-embedding, as happens on human biopsies routinely. Did the author compare the heights of the villi to the depths of the crypts for control purposes? Or for that matter, the relative thickening of crypt layer and gland layer? Of course not! Your instructor wrote to Lancet (who turned down my letter) and to the author (Arpad Pusztai, who had gone on TV and made inflammatory statements about the public being used as guinea pigs; he didn't respond either and is now a leading antibiotechnology activist and celebrated "persecuted genius"). Lancet ended up admitting (May 29, 1999) that it knew the paper was junk science when it was published but that if it hadn't published it, it would have been smeared for "suppressing information" by anti-biotechnology militants. I am not making any of this up. Regrettably "environmental activism" is built largely on this kind of stuff. As late as 2005, Greenpeace USA's website was still citing the paper as the strongest proof of the dangers of bioengineered food ("damaged immune systems and stunted growth of vital organs"), and it's still cited by several thousand anti-biotechnology pages all over the internet (2012).
* The mucosa protects itself with a host of protease-inhibitors, phospholipids, glycoproteins, etc., etc.; neutrophils and lots of other things damage it (Dig. Dis. Sci. 39: 138, 1994), etc., etc. You'll go crazy trying to keep them all straight.
INTESTINAL METAPLASIA (review Gut 52: 1, 2003):
A common finding. Most often it's caused by helicobacter. It's seen in both in autoimmune atrophic gastritis with achlorhydria and in multifocal non-autoimmune atrophic gastritis. It's seen in the presence of bile reflux and when there has been previous radiation.
An experienced endoscopist can spot areas of intestinal metaplasia by their slightly more whitish color.
Intestinal metaplasia is clearly the precursor lesion for "intestinal type" stomach cancer.
TYPE I:
Straight crypts, regular architecture, mature enterocytes, Paneth cells, and goblet cells, neutral mucin
{15432} type I intestinal metaplasia (right)
{15534} type I intestinal metaplasia
TYPE II:
Mild distortion of glands, few enterocytes or Paneth cells, many mucin-producers and goblet cells, neutral mucin, * carboxymucin
TYPE III:
Variable degrees of glandular distortion, cells less differentiated, mostly sulfo-mucin ("colonic differentiation").
Any kind of stomach cancer can harbor any kind of mucin. In case somebody (not me) asks:
SULFOMUCIN... Very acid... Intestine; if in stomach, the epithelium is atrophic-metaplastic and is likely to turn nasty; may not even be PAS positive (?)
CARBOXYMUCIN... Acid... Intestine (also called "acid sialomucin")
NEUTRAL MUCIN... Neutral... Stomach (also called "neutral sialomucin").
Future pathologists: Use alcian blue to stain the acid mucins!
I am almost sorry to have to add that all three types may represent either multistep-mutations-of-carcinogenesis or just tissue regeneration (Cancer 74: 556, 1994); the distinction is of no importance (J. Clin. Path. 54: 679, 2001). This is sad because during the 1990s, we pathologists honed our color-vision to distinguish normal gastric neck cells from "small-intestinal type" intestinal metaplasia, etc., etc.
* Stay tuned for prognosticating "intestinal metaplasia", judging whether it is reversible upon eradicating helicobacter (consensus is now that this is the norm: Gut 54: 1536, 2005), based on gene studies (Gut 52: 1, 2003) and/or immunostaining and/or repeat endoscopy (Dig. Dis. Sci. 45: 1754, 2000). "Das-1 positive is premalignant" (Gut 52: 80, 2003).
BIRTH DEFECTS
DIAPHRAGMATIC HERNIAS result from failure of the diaphragm to form properly. Portions of stomach, intestines, and other organs end up in the chest.
{15607} diaphragmatic hernia, left leaf never formed
{49138} diaphragmatic hernia, left leaf never formed
Congenital (HYPERTROPHIC) PYLORIC STENOSIS is probably a hereditary defect of variable penetrance in which the pylorus of the stomach is hypertrophic, and the gastric outlet may become fully obstructed, typically at the end of the first month of life. The infant experiences projectile vomiting, and the surgeon feels a mass ("feels like an olive") in the upper abdomen. Surgical splitting of the pylorus effects a cure.
It is more common in boys, and Turner's XO is also a risk.
* Old claims of simple inheritance failed, but there is a familial tendency (JAMA 303: 2393, 2010).
* More recently, the understudied "interstitial cells of Cajal", little cells that have a lot to do with pacemaking for gut motility, have been found to be somewhat lacking both in numbers and a key enzyme in the pylorus in these kids (Arch. Path. Lab. Med. 127: 1182, 2003). Stay tuned.
* Less common...
It's not rare to find a bit of ectopic pancreas.
You may also find lung, complete with bronchus -- the famous "pulmonary sequestrum." It's harmless.
DIEULAFOY'S MALFORMATION is an extra-large artery running along the mucosa of the lesser curvature. It can cause severe bleeding, even into the chest (Chest 110: 567, 1996; Ann. Thorac. Surg. 80: 1126, 2005).
Often impressive. Causes include beer chug-a-lugging, bowel obstruction, misplaced endotracheal tubes, gastroparesis (think of diabetic autonomic neuropathy), and (in the dead) inept CPR attempts. (Amateurs first blow air into the stomach, then rupture it by pressing in the wrong place. See Ann. Int. Med. 30: 343, 1997.) {49141} gastric dilatation |

|
BEZOARS
These are swallowed goodies that remain permanently in the stomach.
Hairballs (TRICHOBEZOARS) are seen in people who enjoy nibbling their long hair ("Rapunzel syndrome"). Or ask a pet cat. Review Mayo Clin. Proc. 73: 653, 1998. Pharmacobezoar (pill collection in the esophagus -- "so that's why they didn't work"): Eur. Assoc. Poison 49: 348, 2011; Clin. Tox. 49: 72, 2011.
![]() Yarn bezoar
Yarn bezoar
Yutaka Tsutsumi MD
PHYTOBEZOARS may be chunks of ill-chewed vegetable matter, or (worst) persimmon remnants. The latter contain a substance that, complexed with acid, turns into cement and may require surgery.
Things that interfere with gastric emptying (diabetes, other dysautonomias, post-vagotomy, anti-cholinergic medicines) enhance one's ability to personally experience a bezoar.
{49150} bezoar
{10160} trichobezoar
ACUTE GASTRITIS: Acute damage to the gastric mucosa from any cause.
If there is necrosis of any epithelial cells, it is "erosive gastritis" -- you remember that an erosion is inflammation plus necrosis of an epithelium without necrosis of the underlying connective tissue (at least not yet).
Pathogenetic mechanisms include:
"Big Robbins" listed, or could have listed, these important causes:
![]() Eosinophilic / allergic gastroenteritis
Eosinophilic / allergic gastroenteritis
Joel K. Greenson MD
U. of Michigan
|
|
![]() Helicobacter pylori
Helicobacter pylori
Joel K. Greenson MD
U. of Michigan
You can figure out for yourself what the mechanisms might be in each case. Anatomically, you may see anything from mild edema and a few polys to bloody sloughing of chunks of the upper mucosa, and symptoms can range from "upset stomach" to vomiting blood by the pint.
AUTOIMMUNE ("FUNDIC", "DIFFUSE ATROPHIC", formerly "TYPE A") CHRONIC GASTRITIS is an autoimmune process that attacks primarily the fundic glands.
You'll see loss of mucous secretion, striking shortening of the glands, and usually loss of the parietal cells.
Patients usually (60+%) have autoantibodies against parietal cell H+/K+ ATPase (and usually others against intrinsic factor). This is the usual cause of the achlorhydria (i.e., greatly diminished or no stomach acid) and classic "Addisonian" pernicious anemia. JAMA 278: 1946, 1997; update Gastroenterology 120: 377, 2001.
Around 10% of these patients go on to develop stomach cancer.
Many of these patients have other autoimmune endocrine diseases as well. The three to remember are Addison's disease of the adrenals, Hashimoto's disease of the thyroid (Arch. Int. Med. 159: 1726, 1999), and insulin-dependent diabetes.
Future pathologists: Since there is no acid and no feedback, the G-cells undergo hyperplasia in the antrum. They are a single layer of clear cells. This is a breeding-ground for carcinoids. Yes, really, the lack of acid greatly increases the risk. This is important as "lack of acid causing carcinoid" is a medicolegal concern if you recommend long-term antacids.
Work on autoimmune gastritis is overshadowed nowadays by helicobacter, but the finding of anti-parietal cell autoantibodies seems solid. Perhaps those lacking the antibody were really helicobacter-induced atrophy (see below). And helicobacter itself can evidently trigger the autoantibodies (I was surprised, too: Gastroent. 115: 340, 1998) by molecular mimicry (Inf. Imm. 64: 2031, 1996). Update: Blood 107: 1673, 2006.
![]() Pernicious anemia
Pernicious anemia
Immunoglobulin on parietal cells
WebPath Photo
{15426} "atrophic gastritis", gross
{15434} "atrophic gastritis"
{15561} early atrophic gastritis, starting on surface
HELICOBACTER GASTRITIS is a serious problem worldwide.
As you know, Marshall and Warren of Australia won the Nobel Prize in 2005 for discovering the importance of Helicobacter. You'll learn the story in your microbiology course.
Of course, most are H. pylori. * The zoonosis H. heilmannii is much less common and gives pretty much the same picture, generally with lots of lymphocytes (J. Cln. Path. 54: 774, 2001; Am. J. Surg. Path. 29: 1537, 2005).
The vast majority of the old "type B / environmental chronic gastritis" (now "multifocal atrophic gastritis") cases are caused by helicobacter that's still present. You'll have no trouble recognizing the familiar wiggly creatures on the surface of (often obviously damaged) gastric mucosa. Giemsa, immune, or silver stains show them to advantage.
Helicobacter flourishes in the stomach because it cleaves urea to ammonia, neutralizing the strong acid that would otherwise surround it (Science 287: 482, 2000). Helicobacter's first virulence factor, CagA protein, actually gets inoculated into the stomach cells (Science 287: 1497, 2000). How it does its damage is just now being worked out (Dig. Dis. Sci. 58: 1830, 2013). The second virulence factor, VacA (vacuolizing cytotoxin A) is even more mysterious.
The antrum is most severely involved when helicobacter is present. There's a chronic infiltrate with both lymphocytes and neutrophils. (Ordinarily, you'll see plasma cells in the stomach mucosa, but lymphocytes should be very few.) The neutrophils tend to be in the neck region of the glands. Lymphoid follicles, or even little groups of lymphocytes, in the mucosa suggest "Helicobacter"; when very abundant, they produce "nodular gastritis" which runs a continuum into "helicobacter lymphoma." Pyloric metaplasia advances from the antral area into the fundus, perhaps decreasing acid production, and the fundic glands may atrophy as well. You may see intestinal metaplasia, especially near any ulcers that may be present. Acid production may be increased, decreased, or normal.
An endoscopist can recognize atrophic mucosa by its thinning and loss of good rugae and can biospy it. Today, we distinguish "multifocal atrophic gastritis" (helicobacter has always been present, fundus and antrum are always unevenly involved, autoimmunity is not the primary problem, some parietal cells are still present though acid production may be decreased) and "autoimmune atrophic gastritis" (helicobacter is probably the trigger but may not be presnt, the fundus is completely involved but the antrum is spared, there's often antibodies against intrinsic factor and/or parietal cells, and there's achlorhydria and a risk for pernicious anemia). The glands are always shortened (from just a little to a lot), and both illnesses generally show intestinal metaplasia. Both are precursor lesions for stomach cancer.
In any portion, the rugae are likely to flatten and vanish. The process begins at the surface and work downward into the glands. Lesions of various stages are present simultaneously in different parts of the stomach. Eventually, the surface will come to exhibit at least some intestinal metaplasia and probably some degree of dysplasia.
Removing helicobacter cures this illness (J. Clin. Path. 4: 22, 1994).
The third pattern of helicobacter infection is "non-atrophic antral-predominant gastritis", which usually correlates with gastric and/or duodenal ulcer rather than stomach cancer. Most people with significant duodenitis (i.e., polys in the epithelium, usually gastric metaplasia and extra plasma cells) have helicobacter gastritis (Am. J. Clin. Path. 90: 711, 1988, kids Am. J. Clin. Path. 102: 188, 1994 & Dig. Dis. Sci. 39: 1488, 1994), etc., etc.
* Don't worry about the fourth pattern -- non-atrophic corpus-predominant gastritis, in people on proton pump inhibitors.
|
|
|
|
|
|
{11728} Helicobacter in gastritis (look close)
{15440} Helicobacter
{19492} type B, antrum
{19491} type B, antrum
{26903} type A
{26906} type A
{26909} type A, some atypia
|
|
|
OTHER FORMS OF GASTRITIS: /
* LYMPHOCYTIC GASTRITIS features lymphocytes actually in the epithelium itself. It's usually a surprise; patients may have helicobacter, sprue, or neither (Am. J. Surg. Path. 23: 153, 1999). Nowadays we define it to be helicobacter-negative.
MENETRIER'S DISEASE ("idiopathic hypertrophic gastritis"; "enlarged fold gastitis"): Idiopathic hyperplasia of the surface mucous cells, with corresponding atrophy and twistiness (tortuosity) of the glands and loss of the parietal cells and acid production. Vomiting, diarrhea, and protein loss are likely to be severe. Makes for some big folds, and a lot of protein loss in the excessive mucus. Intestinal metaplasia and neoplasia may supervene. Today, the pathologist must see decreased parietal cells as well as dilated, tortuous glands and foveolar hyperplasia (Gut 59: 1617, 2010). There may be eosinophilis and/or hyperplasia of smooth muscle (Gut 59: 1617, 2010).
Menetrier's is caused (at least sometimes) by helicobacter, and resolves when you clear the bacteria (Gut 35: 701, 1994). Growth factors producing the huge folds: Gut 39: 787, 1996. The strain of helicobacter seems to be the reason: Dig. Dis. Sci. 53: 1785, 2008.
{19486} Menetrier's, gross
{19487} Menetrier's, histology
ZOLLINGER-ELLISON SYNDROME: Gastrinoma (often in the pancreas) causing hyperplasia of the gastric glands. Makes for a very upset, ulcerated stomach.
* GRANULOMATOUS GASTRITIS: Sarcoid, Crohn's, idiopathic (for the latter see J. Clin. Path. 63: 347, 2010). All are non-caseating, of course.
STRESS ULCERS (the usual "acute erosions") are small (less than 1 cm) areas of loss of some (or all) the mucosa. Note that nobody really knows where "acute gastritis" leaves off and "stress ulcers" begin; probably they're part and parcel of the same reaction pattern.
Nomenclature: If the patient has burns, they are "Curling's ulcers" (* think of a hot curling iron). If the patient has intracranial trauma, they are "Cushing's ulcers" (attributed to vagal stimulation of gastric acid secretion, named for famous neurosurgeon Harvey Cushing).
Their pathogenesis constitutes a major mystery of medicine. Except in Cushing's ulcers, hyperacidity does not seem to be the problem. Most of the factors that produce "acute gastritis" can also help produce stress ulcers. Some workers now favor catecholamine effect (i.e., ischemia) and/or some glucocorticoid effect.
Pre-pyloric erosions are due to stress (Scan. J. Gastr. 24: 522, 1989).
{15425} "stress ulcer", gross
{18711} "stress ulcers", gross
{19350} "gastric erosion", histology
{39426} hemorrhagic gastritis, nasogastric tube erosions
{07184} hemorrhagic gastritis, nasty case
* A sweet-and-simple test for the integrity of your gastric mucosa: swallow some sucrose and test for sucrose in the blood! Lancet 343: 998, 1994.
|
|
|
|
|
{10471} benign stomach peptic ulcer
{15438} benign stomach peptic ulcer
{15439} benign stomach ulcer, with clot
{15560} histology of ulcer, arrow marks bleeding point
{19372} peptic ulcer
{26888} peptic ulcer, stomach
The familiar "ulcer" of stomach or duodenum. Ulcers resulting from the digestive action of acid-pepsin ("no acid, no ulcer") on the gastric mucosa. A common problem, somewhat more common in men, usually subclinical, prone to remit and relapse ("once an ulcer, always an ulcer"). "Ulcers" can occur anywhere along the GI tract. Frequency:
80% duodenum
19% stomach
1% elsewhere
Risk factors for ulcer include...
You WILL get an ulcer, and probably several, if you develop a gastrinoma.
Ask a gastroenterologist about the differences among ulcer patients.
Those with duodenal ulcers tend to secrete acid too abundantly when stimulated, and to empty their stomachs too readily.
Gastric ulcer types tend to have low-normal levels of acid, and tend either to have chronic gastritis or take lots of aspirin or other substances noxious to the stomach. People with longstanding gastric ulcers almost all have "chronic gastritis" in the antrum, and intestinal metaplasia near the ulcer.
![]() NSAID Gastritis
NSAID Gastritis
Joel K. Greenson MD
U. of Michigan
* Whether or not helicobacter is on board, gastric ulcers seem to be preceded by abnormalities of the phospholipids in the gastric epithelium, with loss of their normal protective function. This may be a common pathway by which helicobacter, atrophic gastritis, cirrhosis, certain animal models, and others produce ulcer (Gastroent. 107: 362, 1994).
Most patients with duodenal ulcers, and a majority of those with gastric ulcers, now are known to have helicobacter, and the bug must be an important part of the pathogenesis.
The early wisdom was that almost everybody with a gastric or duodenal ulcer has helicobacter on board (Gut 35: 19, 1994), and eliminating the creature eliminates the disease. Of course that was an exaggeration. It's well-established that a large minority of stomach ulcer patients are helicobacter-negative (Gastroent. 128: 1845, 2005).
In the duodenum, there appears to be a vicious cycle between helicobacter infection and antral metaplasia (J. Clin. Path. 43: 981, 1990, Am. J. Clin. Path. 102: 188, 1994) that permits the bugs to thrive. This is not surprising, considering the abrupt appearance and disappearance of ulcers. Antral metaplasia is a common finding in normal duodenum (Am. J. Clin. Path. 90: 711, 1988), and perhaps this how duodenal ulcers begin.
The rare helicobacter-negative duodenal ulcer patient may have Crohn's, Zollinger-Ellison, taking steroids, bisphosphonates or NSAID's (review Gut 35: 891, 1994; nobody knows how it works), or just be unlucky (Gut 34: 762, 1993; Am. J. Med. 91: 15, 1991).
Peptic ulcers are usually single, and most are less then 3 cm across. They look sharply punched-out (as you'd expect, rolled borders suggest malignancy). However, they may penetrate deeply. The base is always keep clean by digestive juice. Gastric ulcers are usually on the lesser curvature, and the favorite site is near or in the antrum. Duodenal ulcers are usually in the first portion, but may be anywhere. As scar contracts, the mucosal folds radiate from the ulcer.
Peptic ulcers may cause pain (relieved when food or antacid neutralizes stomach acid, recurring after a meal stimulates stomach acid), hemorrhage, perforate (call the surgeon!) and/or cause fibrosis leading to obstruction (notably of the pylorus). We believe they do not undergo malignant transformation ("cancers often ulcerate, but ulcers seldom/never cancerate").
Future surgeons: You may "CHOP" out the ulcer if it is Chronic, Hemorrhaging uncontrollably, Obstructing the gastric outlet, or Perforated.
BENIGN TUMORS
HYPERPLASTIC POLYPS ("inflammatory polyps"; Dig. Dis. Sci. 54: 1839, 2009) are extremely common and thought to result from exuberant regeneration of the mucosal epithelium -- you don't see them in normal stomach, and usually there is helicobacter around. They usually look like multiple little rice grains, but may be larger. Microscopically, they are composed of dilated glands lined with pit-type cells.
The big ones (over 1.5 cm) can turn cancerous (Dig. Dis. Sci. 41: 377, 1996). Even the little ones may show a bit of dysplasia; no one knows their natural history for certain but nobody really worries about malignancy.
{09292} hyperplastic polyps of stomach
{38656} hyperplastic polyps of stomach
![]() Gastric hyperplastic polyp
Gastric hyperplastic polyp
Wikimedia Commons
FUNDIC GLAND POLYPS are very common bumps; on biopsy, the pathologist sees shortened pits and cystic change of the glands. They probably have little or no malignant potential (Dig. Dis. Sci. 48: 1292, 2009).
Their presence has also been attributed to chronic use of proton pump inhibitors. This is now pretty well established (Dig. Dis. Sci. 56: 1743, 2011). How could this happen?
* INFLAMMATORY FIBROID POLYP is a mass of vessels and stroma looking like granulation tissue, plus a lot of eosinophils. It's usually a submucosal lesion in the gastric antrum. Don't worry about the special stains we use to make the call.
* JUVENILE POLYPS resemble those we'll meet later in the colon.
ADENOMATOUS POLYPS ("neoplastic polyps", "intestinal type polyps", or just plan "adenomas") tend to be pedunculated, with villi and/or crypts, and the current definitions require some dysplasia as we'll see later in large-intestinal polyps. They are premalignant, there is a link to syndromes and a familial tendency, and maybe half would turn into cancer if left alone (but who wants to do that study?)
* Foveolar adenomas look similar but have "foveolar dysplasia" instead. Don't worry about them.
* There are a few other types of stomach adenomas; don't worry about them.
{09333} adenomatous polyp
{09312} adenomatous polyp
{09331} adenomatous polyp
![]() Adenomatous polyp
Adenomatous polyp
Ed Uthman MD
Wikimedia Commons
* Grading is undergoing revision. Here's one grading system:
* There is now a staging system (Cancer 117: 4916, 2011).
* Some GI stromal tumors do not light up for "kit"; they tend to have mutated PDGFRA, or neither gene mutated (these usually have mutated BRAF or succinate dehydrogenase), and do not respond to imatinib. More about predicting responses to targeted therapies for these tumors: Arch. Path. Lab. Med. 136: 483, 2012.
{09299} leiomyoblastoma
* Subclassifying them: Ann. Surg. 242: 64, 2005. Those resulting from atrophic gastritis almost never kill, other types are more aggressive. Here's a popular system:
GASTRIC ADENOCARCINOMA (common "stomach cancer"; Lancet 362: 305, 2003; Ann. Surg. 241: 27, 2005)
While its prevalence in the U.S. decreased strikingly between the beginning and the end of the 20th century, this continues to be an important cancer killer in every country. Around 15,000 people per year die of stomach cancer in the U.S. Rates in the rest of the world are also declining (J. Clin. Path. 61: 172, 2008 -- includes "best practice" for pathologists grossing-in stomachs). Right now, rates are highest in Chile (where it's always been extremely common for some reason), Peru, and Russia.
Risk factors include:
Diet and environment are evidently much more important than ethnic background. First-generation immigrants have the risk of their home countries; second-generation immigrants the risk of their new countries (Ann. Surg. 241: 27, 2005).
The Lauren classification (which is the more-useful one; the WHO classification less so) distinguishes two major types of gastric adenocarcinoma, with different cells of origin.
(1) DIFFUSE INFILTRATIVE GASTRIC ADENOCARCINOMA arises from the neck cell.
Evidently autoimmune gastritis, and intestinal metaplasia are not risk factors. It's less strongly linked to helicobacter than the more common stomach cancers, but the old story about helicobacter not being a risk factor at all is probably not so (World J. Gastroent. 11: 1387, 2005).
The frequency of this cancer is actually increasing again in the US (CDC: Arch. Path. Lab. Med. 128: 765, 2004). No one knows why.
* Hereditary diffuse gastric adenocarcinoma, an anti-oncogene deletion syndrome, is caused by mutated E-cadherin (CDH1): Gut 53: 814, 2004; JAMA 297: 2360, 2007. Signet-ring cancers begin at the body-antral junction, and are already invading the upper mucosa long before they are visible on endoscopy. Prophylactic gastrectomy seems like a good idea (confirmed Cancer 112: 2655, 2008); management Am. J. Surg. Path. 36: 1709, 2012.
(2) INTESTINAL TYPE GASTRIC ADENOCARCINOMA typically arises in the setting of longstanding "atrophic gastritis" or other "chronic gastritis", usually in the presence of helicobacter and/or autoimmune gastritis and/or intestinal metaplasia and/or bile reflux.
This is the kind of cancer that's usually seen where the disease is very common. Mostly it's a disease of older folks.
Helicobacter produces epithelial hyperproliferation. We are starting to learn about the molecular biology and virulence factors behind this (Gastroenterology 141: 553, 2011).
As in the esophagus, men are more at risk because women get the disease later (Gut 58: 16, 2009). It features large glands made of tall cells with rod-shaped nuclei (as in the more common, more familiar primary carcinomas of the colon). This is the common type of stomach cancer in the high-risk countries.
How we discovered the link to helicobacter: Am. J. Clin. Path. 100: 236, 1993); Cancer 73: 2691, 1994; Cancer 75: 2203, 1995; Dig. Dis. Sci. 41: 950, 1996. Does eradicating helicobacter prevent progression of intestinal metaplasia to cancer? Yes! Gut 53: 1244, 2004. No! JAMA 291: 187, 2004.
* You'll go crazy trying to guess how helicobacter causes stomach cancer. One idea (epigenitically, by methylation, silencing trefoil factor 2, which causes repair and prevents neoplasia) is outlined in Gastroenterology 139: 2005, 2010. In any case, we have enough experience by now to know that eradicating helicobacter does reduce your long-term risk for stomach cancer (Ann. Int. Med. 151: 121, 2009).
* News: Around half of stomach cancers arising in the gastric cardia (but not elsewhere) probably arise from Barrett's esophagus (Arch. Surg. 129: 609, 1994); these are the least-likely common cancers to be helicobacter-linked. Despite older claims, cancer of the cardia doesn't seem to differ substantially in terms of risk factors or behavior (J. Am. Coll. Surg. 206: 306, 2008), and pathologists are only now working out markers to tell them apart, which is generally moot in any case.
* Some cancers, espsecially after partial gastrectomy,
are rich in lymphocytes and these are almost always loaded with
actively-produced Epstein-Barr
virus![]() (Cancer 74: 805, 1994). Similar tumors are common
in the Far East regardless of previous surgical procedures.
Stomach cancers "with lymphoid stroma"
are less aggressive than common gastric cancers (Arch.
Surg. 129: 615, 1994), even if they are not the result of
previous surgery, and regardless of Epstein-Barr positivity (the virus is usually
present). Histopathology 36: 252, 2000; molecular biology
Gastroent. 121: 612, 2001; Am. J. Path. 161: 1207, 2002;
Am. J. Clin. Path. 121: 237, 2004.)
(Cancer 74: 805, 1994). Similar tumors are common
in the Far East regardless of previous surgical procedures.
Stomach cancers "with lymphoid stroma"
are less aggressive than common gastric cancers (Arch.
Surg. 129: 615, 1994), even if they are not the result of
previous surgery, and regardless of Epstein-Barr positivity (the virus is usually
present). Histopathology 36: 252, 2000; molecular biology
Gastroent. 121: 612, 2001; Am. J. Path. 161: 1207, 2002;
Am. J. Clin. Path. 121: 237, 2004.)
The gross is the usual for a cancer (a cauliflower, an ulcer, or -- especially in the signet-ring type -- diffuse invasion). The histology is what you'd expect. In either case, you may see invasive glands, papillae, signet-ring cells, mucus lakes, desmoplasia, and most anything else, though when you see signet ring cell invasion, it is usually the "diffuse" type rather than the "intestinal" type. Signet-ring cells in stomach cancer, as in esophageal cancer, in particular denote a bad prognosis (Ann. Surg. 250: 878, 2009). Terms: LINITIS PLASTICA: "leather bottle" stomach from a diffusely-infiltrating, desmoplastic cancer. KRUKENBERG TUMOR: Drop-metastases causing enlargement of the ovaries. SISTER MARY JOSEPH'S NODE: metastasis to the umbilicus (named for the Mayo brothers' scrub nurse). RECTAL SHELF ("of Blumer"): Drop-metastases to the lowest place on the peritoneum (remember the "pouch of Douglas"?)
* Grading stomach cancer is based on whether the cancer makes tubules and/or mucus (Goseki I-IV): Gut 35: 758, 1994; some studies claim this gives no useful prognostic information beyond the stage; Cancer 88: 2114 & 2426, 2000 did find it to be of some help.
Symptoms are also what you'd expect -- nausea, vomiting, early satiety, GI bleeding. As you'd also expect, there are usually no symptoms until it's too late. (If you have an extra cauliflower in your stomach, you'd never know it.) There has historically been so much stomach cancer in Japan that people get endoscoped routinely in search of it, and there are many cures (unlike in the US). (For some reason that no one understands, the Japanese have a tremendously high rate of atrophic gastritis, conceivably from the local strains of helicobacter, and this is where most of these cancers arise: Gut 55: 1545, 2006). Biopsy all stomach ulcers you see -- even a cancer may shrink on a regimen of H2-blockers and antacids.
|
|
|
|
|
|
|
|
|
{17511} Stomach cancer, exophytic
{10472} Stomach cancer, ulcerated
{15509} Stomach cancer, linitis plastica, gross
{15562} Stomach cancer, linitis plastica, histology
{08818} Stomach adenocarcinoma, intestinal type
{17517} Stomach adenocarcinoma, intestinal type
{10473} Stomach adenocarcinoma, diffuse type
{39380} Stomach adenocarcinoma, diffuse type
{39392} Stomach adenocarcinoma, diffuse type
{15510} Signet ring stomach cancer
{19346} Stomach cancer, superficial
Most gastric adenocarcinomas are probably preceded by carcinoma-in-situ / high-grade dysplasia (see Arch. Surg. 140: 644, 2005; current thinking is that dysplasia usually invades the mucosa soon, and until it penetrates the muscularis propria, it's called "early gastric cancer" (EGC).
* If you are truly hard-core, here are the four types of dysplasia you may meet in the stomach:
Some diffuse-infiltrating cancers may start de novo, without dysplasia.
{15443} early stomach cancer
Detected late (and it still usually is), stomach cancer has a generally poor prognosis.
{15441} non-metaplastic dysplasia
{15444} non-metaplastic dysplasia
The mainstay of therapy for stomach cancer is still surgery.
* Serum tumor markers: CA 19-9, CA 72-4. Am. J. Surg. 169: 595, 1995. These have proved worthless for screening. There is a new scoring system for HER2/new immunochemistry; maybe 20% are positive and might responsd to trastuzumab (Arch. Path. Lab. Med. 136: 610, 2012).
STOMACH LYMPHOMAS (and other GI lymphomas) are less common than carcinomas but have a better prognosis. Since they tend to be bulky, patients present with obstruction.
WESTERN ("American") LYMPHOMAS are usually B-cell lymphomas (diffuse B-cell or MALT-omas, diagnosable by today's high-tech pathologists). Helicobacter has been established as the big risk factor for both: J. Clin. Path. 47: 437, 1994, J. Clin. Path. 47: 436, 1994; Lancet 345: 26, 723, 724 & 798, 1995 (no surprise, since helicobacter makes lymphoid follicles grow). These lymphomas usually cannot continue to grow without the T-cells directed against the helicobacter (!!! J. Path. 178: 122, 1999). Eradicating helicobacter is curative for most of these, and most of those that don't respond completely are curable with chemotherapy. Some gastric lymphomas are helicobacter-negative and different genetically (Gut 52: 641, 2003).
* MEDITERRANEAN LYMPHOMA occurs especially around the Near-East, features plasmacytoid differentiation and production of alpha-heavy chains ("alpha heavy chain disease.")
SPRUE-ASSOCIATED LYMPHOMA exhibits T-cell markers (reviews Gut 49: 804, 2001; Am. J. Clin. Path. 127: 701, 2007; the more anaplastic primary small bowel lymphomas tend to be preceded by celiac sprue while the less anaplastic ones don't); no one really knows whether complying with the difficult gluten-free diet prevents lymphoma (Arch. Path. Lab. Med. 132: 1594, 2008). The prognosis is generally poor (Blood 118: 148, 2011).
* PSEUDOLYMPHOMA of the stomach is an old term that has no meaning in light of today's molecular diagnostic techniques (Cancer 79: 1656, 1997). You can't always tell severe chronic inflammation from true lymphoma just on histopathology, but today's biotech resolves even the toughest calls by demonstrating clonality (Gut 55: 782, 2006). New twist: There's a NK-cell pseudolymphoma that's very tough to diagnose (Blood 116: 5631, 2010).
![]() Helicobacter lymphoma
Helicobacter lymphoma
Joel K. Greenson MD
U. of Michigan
![]() Lymphocytic gastroenteritis
Lymphocytic gastroenteritis
Joel K. Greenson MD
U. of Michigan
The one really common problem you will see in the DUODENUM is peptic ulcer, already discussed above.
* A "brenneroma" is a curious hamartoma of the duodenum, composed of Brenner's glands and fat.
CANCER OF THE AMPULLA OF VATER is rare and presents clinically as if it were an early cancer of the head of the pancreas.
It's often curable with the Whipple procedure. More about this later.
![]() Ampullary carcinoma
Ampullary carcinoma
Joel K. Greenson MD
U. of Michigan
![]() Ampulla
Ampulla
"Pathology Outlines"
Nat Pernick MD
SMALL INTESTINE
The whole nine yards! -- Ed
|
|
|
You'll cover HOOKWORM, a terrible plague among the shoeless in the Old South and much of today's world, under "Infectious disease." Remember these creatures thrive in the duodenum (especially the Old World hookworm -- Ancylostoma duodenale) and small bowel, and drain blood copiously.
The would-be small-bowel pathologist must be able to recognize three distinct patterns of "villous atrophy".
|
|
BIRTH DEFECTS
You'll learn about exotic malrotation syndromes and reduplication anomalies on "pediatric surgery".
ATRESIA and STENOSIS of portions of the gut probably result from poor vascular flow during embryogenesis. Duodenal atresia patients often have Down's.
Wide-mouth pseudodiverticula off the duodenum can be havens for bacteria (a variant of "blind loop") which can supposedly interfere with absorption especially of vitamin B12.
{53768} duodenal atresia
|
|
|
Pancreatic CHORISTOMAS are little curiosities that may be biopsied to rule out a tumor.
DIVERTICULA, as we've mentioned, are not uncommon in the duodenum, where they may fill with bacteria that get first pickings on foodstuffs, but they are uncommon farther down except for Meckel's.
{18709} diverticulosis, duodenum
{11111} diverticulum, duodenum
Persistence of the omphalomesenteric duct as MECKEL'S DIVERTICULUM (2% of people, two inches long, two feet proximal to the ileocecal valve, 2 types of choristomas -- antral and pancreatic, 2x2 complications -- painful ulcers, bleeding ulcers, "appendicitis", volvulus.)
{10157} Meckel's
{10459} Meckel's
{15563} Meckel's
{38674} Meckel's
![]() Red infarct of the colon
Red infarct of the colon
Neglected peritonitis with
vascular compromise
VASCULAR DISEASE OF THE BOWEL
Despite its abundant vascular supply, the bowel often suffers damage from lack of blood.
TRANSMURAL INFARCTION
Severe, abrupt compromise of the mesenteric circulation will cause necrosis of the bowel. This is always hemorrhagic (why?)
The small intestine is much more vulnerable, since the colon can receive some accessory supply and drainage from its retroperitoneal portions. Even so, the process must be severe, since there's great collateral circulation throughout the bowel.
CAUSES OF BOWEL INFARCTS (transmural or less):
(Obviously this will be acute only when there is some superimposed problem, i.e., thrombosis, rupture into a plaque, shock, congestive heart failure)
After 3-4 days, the gangrenous bowel will perforate. Ischemic necrosis of the bowel is often missed clinically, to everyone's eventual dismay.
Future pathologists: As in any red infarct, the vessels will be dilated and engorged with blood by the time you get the specimen.
MUCOSAL INFARCTION ("HEMORRHAGIC GASTROENTEROPATHY")
When the hypoperfusion of the gut is less severe, only the inner lining of the bowel will die, and the muscular wall and serosa will remain intact.
Usually this results from shock. Remember that digitalis, norepinephrine, and dopamine ("great for keeping the kidneys open") all shunt blood away from the gut. Many long-distance runners have experience with GI bleeding because of diversion of blood from guts to muscles.
Patients have pain, bleeding, etc. As long as the muscularis propria is spared, the lesions are completely reversible.
|
|
{15515} ischemic enteritis, gross
{15538} ischemic enteritis, histology
{19519} ischemic colitis, gross
{49211} ischemic colitis, gross
CHRONIC ISCHEMIA will cause fibrosis and narrowing of the affected portions of bowel. These people may have "intestinal angina" after meals.
No one knows where to put CHRONIC NONSPECIFIC MULTIPLE ULCERS of the small intestine, or the almost-identical-looking NSAID ENTEROPATHY (long-acting preparations of old-fashioned NSAIDS are notorious), beyond saying that they remain mysterious and cause chronic blood loss (Dig. Dis. Sci. 51: 1357, 2006; Gastroenterology 128: 1172, 2005).
BOWEL INFECTIONS
You'll learn more about these in "Micro". Remember that extensive inflammation of the bowel from any cause produces diarrhea (why?) and protein loss (why?) Many people now say that campylobacter is the most common cause of gastroenteritis. Cryptosporidium, once considered non-pathogenic for humans, is now known to be a very common cause of acute gastroenteritis. Rotavirus (which blocks the proteins that allow absorption of nutrients from the gut, producing an osmotic diarrhea) is a major killer worldwide. Cyclosporiasis ("the raspberry bug") is another protozoan that may be another major overlooked disease; we now know it's very common in the poor nations (Am. J. Trop. Med. 84: 38, 2011).
Remember that the common diarrheal illnesses (nasty E. coli, viruses) can and do kill people, particularly children. E. coli strain O157:H7 ("enterohemorrhagic E. coli"; "shiga-toxin producing E. coli"; "STEC") of course produces the toxin and a shigella-like illness.
"Enterotoxic E. coli" produces traveller's diarrhea.
Worldwide, diarrhea kills millions of children each year. Current estimate is over half a million deaths from rotavirus, which should be vaccine-controllable (BMJ 336: 751, 2008; update NEJM 360: 1063, 2009; NEJM 362: 358, 2010); works fairly well even in the very poor nations (JAMA 301: 2243, 2009; Lancet 376: 568, 606 & 615, 2010). You'll learn the other bacterial, viral, and protozoal infections in "Micro".
Morphologists:
TB produces ulcers with their long axes perpendicular to the long axis of the bowel (in contrast to the eschar-filled ulcers of typhoid, in which they run parallel.) Popular trivia question.
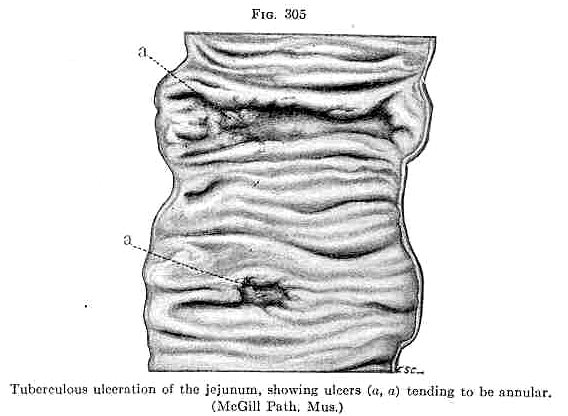 Tuberculosis of the jejunum
Tuberculosis of the jejunum
Classic drawing
Adami & McCrae, 1914
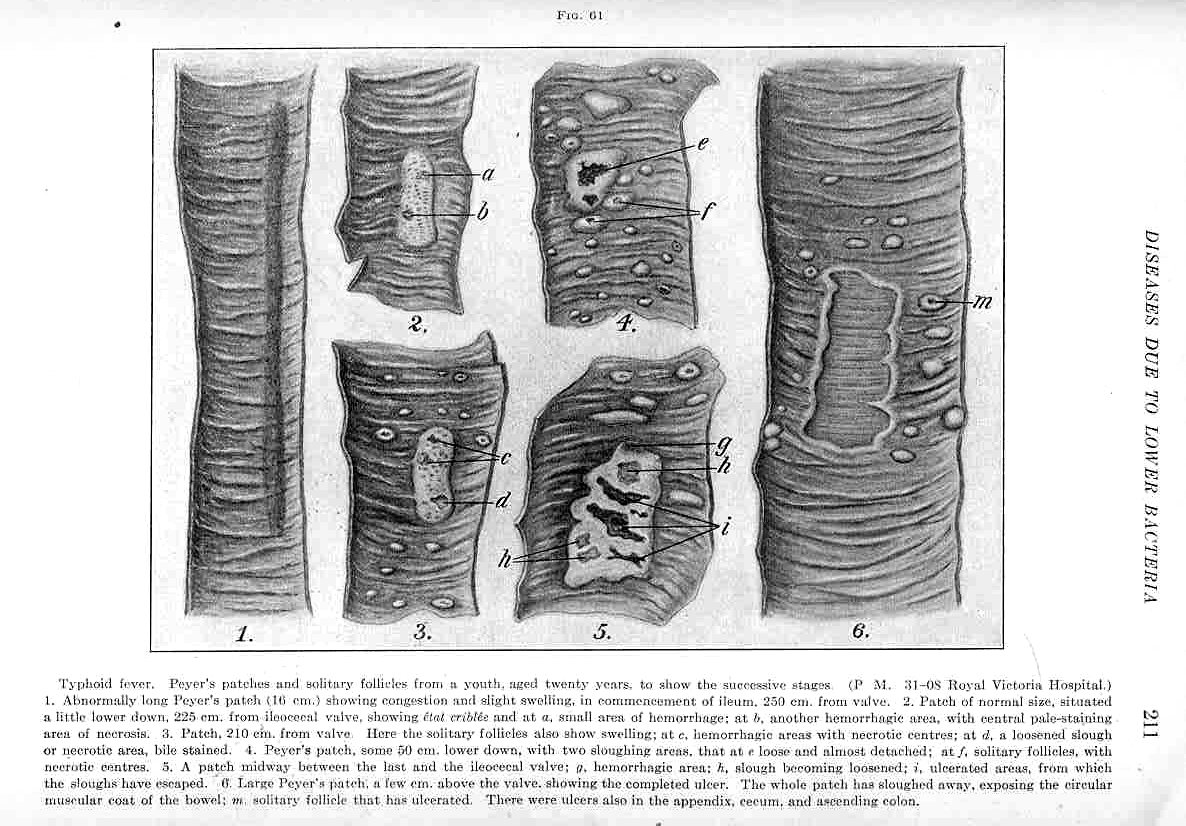 Typhoid ulcers of the intestine
Typhoid ulcers of the intestine
Classic drawing
Adami & McCrae, 1914
Yersinia enterocolitica and Campylobacter jejuni produce granulomas with stellate microabscesses.
Salmonella (typhoid, paratyphoid) infections attract primarily macrophages. Look for erythrophagocytosis.
CHOLERA -- no anatomic pathology apart from the fluid shifts
For more on cholera, click here.
For more on salmonella, click here.
For more on shigella, click here.
For more on typhoid, click here.
Mycobacterium avium-intracellulare -- packed with macrophages filled with acid-fast mycobacteria
Cryptosporidiosis is newly recognized as an important cause of diarrhea. Healthy people can shake the infection; it will linger in the immunodeficient.
![]() Cryptosporidiosis colitis
Cryptosporidiosis colitis
Joel K. Greenson MD
U. of Michigan
* INTESTINAL SPIROCHETOSIS just means a layer of anaerobic spirochetes (Serpulina pilosicoli, Brachyspira aalborgi, maybe others) overlying a slightly damaged surface epithelium, usually in the distal colon and rectum. See J. Clin. Microb. 36: 261, 1998; J. Clin. Microb. 37: 2093, 1999; Am. J. Clin. Path. 120: 828, 2003. Causes abdominal pain and/or diarrhea.
Gourmets:
PEA SOUP STOOL: Typhoid, salmonellosis, other.
CURRANT JELLY STOOL: Inflammatory bowel disease, dysentery (shigella, amoebas); intussusception
RICE-WATER STOOL: Cholera, other enterotoxins
Making the diagnosis:
GRAM STAIN: Staphylococcal colitis![]() (uncommon; you've taken too many antibiotics
and killed off the friendly commensals)
(uncommon; you've taken too many antibiotics
and killed off the friendly commensals)
SMEAR FOR POLYS: Invasive bacteria (shigella, salmonella, yersinia, campylobacter, enteroinvasive E. coli), Crohn's, ulcerative colitis
FRESH MOUNTS: Amoebas, worms, giardia (for this, try a duodenal aspirate), cholera
ELECTRON MICROSCOPE: Viruses.
BIOPSY: CMV![]() ,
herpes
,
herpes![]() ;
graft-vs.-host
;
graft-vs.-host
BLOOD CULTURE: Best way to find typhoid
STOOL CULTURE: Invasive bacteria (shigella, salmonella, yersinia, campylobacter)
ACID-FAST: TB![]() (good luck), atypical mycobacteria, cryptosporidiosis (easy), isospora
(good luck), atypical mycobacteria, cryptosporidiosis (easy), isospora
{09826} acid-fast stain, atypical mycobacteria
SEROLOGY: Typhoid, extra-intestinal amebiasis
TOXIN ASSAY: Pseudomembranous enterocolitis for C. difficile
Classic male GAY BOWEL SYNDROME / PROCTITIS was caused by any of a host of infectious agents,
including amoebas, campylobacter, echovirus, giardia, gonococci,
herpes![]() ,
shigella, salmonella, and
yersinia. With changing life-styles in the AIDS era, the problem became much less common,
but is now reappearing; the usual agents are gonorrhea, syphilis, chlamydia, and herpes
(Dig. Dis. Sci. 57: 269, 2012).
,
shigella, salmonella, and
yersinia. With changing life-styles in the AIDS era, the problem became much less common,
but is now reappearing; the usual agents are gonorrhea, syphilis, chlamydia, and herpes
(Dig. Dis. Sci. 57: 269, 2012).
* We hope we never again see an outbreak of alimentary toxic aleukia. This is caused by eating grain contaminated with the fungal toxin T-2 from Fusarium species. A severe gastroenteritis followed about two weeks after exposure, and aplastic anemia also develops. This killed hundreds of thousands of Russians during World War II.
A systemic disease where ulcers and fibrosis, often with granulomas, affect portions of the alimentary canal. Maybe one person in 1000 is affected; the onset is typically in the teens or in later middle age (two peaks). |  Dwight Eisenhower |
The morphology of Crohn's is distinctive.
Transmural involvement (i.e., all three layers) of the gut is the rule.
The mucosa shows ulcers, which begin as pinpoint lesions ("aphthae") and coalesce into longitudinal, serpentine fissures and cobble-stoning. Later in the disease, or after surgery, these are likely to penetrate deep through the gut wall. They will either perforate or form fistulas skin or other loops of bowel. Healing produces fibrosis of the mucosa.
The wall is edematous and rubbery, progressing to fibrosis ("garden-hose"). The thickening of the wall narrows the lumen (radiologists: "string sign").
The serosa becomes dusky gray and fibrous, and the fat tends to "creep around" the mesentery ("fat wrapping", which helps the surgeon recognize the diseased segments).
In each layer, you will see at least a bit of lymphoid infiltrate. You may see sarcoid-like granulomas (this is the only way, on mucosal biopsy of the large bowel, to prove the disease isn't ulcerative colitis instead). In the small bowel, around 50% of cases have granulomas; it's about the same percent in the large bowel (J. Clin. Path. 60: 1268, 2007).
Most impressive, these lesions are sharply-demarcated from normal regions ("skip lesions").
The most common site of involvement is the terminal ileum.
Since any portion of the gut can be involved, these patients are prone to aphthae in the mouth, fibrosis ("sclerosing cholangitis") of the bile ducts, perianal abscesses, and fissures and fistulas of the anus. The first problem may even be in the vulva (Dig. Dis. Sci. 54: 1565, 2009; Pediatrics 125: e1518, 2010).
The healing epithelium in Crohn's disease may exhibit atypia (dysplasia), but cancer is uncommon (supposedly 2% or so; it behaves as in ulcerative colitis Gut 35: 950, 1994; one study considers careful screening to be in order: Ann. Surg. 223: 186, 1996); colonoscopy does seem to save lives (Gut 44: 580, 1999). Update on colonrectal cancer especially in ulcerative colitis and Crohn's: Ann. Surg. 252: 330, 2010.
* There's some concern about new therapeutic regimens increasing cancer risk (Gastroent. 146: 941, 2014; Am. J. Gastro. 109: 212, 2014); stay tuned.
Despite the well-known anatomic pathology, the etiology remains obscure.
There is an obvious disturbance involving the immune system of the gut. Alterations in the lymphocyte populations are very different from normal, even in fistulas (Gut 53: 1314, 2004), and a tremendous literature exists on immunologic abnormalities but with no unifying mechanism yet clear. The only consensus so far is that the immune system is reacting somehow to gut contents (Lancet 369: 1025, 2007).
Right now, there is much being discussed about various antibodies defining subsets of Crohn's and/or helping distinguish it from ulcerative colitis. Update: Am. J. Gastro. 101: 360, 2006; Gut 56: 1394, 2007.
* Despite decades of trying, and many positive reports,
there's no agreement as to whether mycobacteria are usually
present in the lesions. (A recent claim that they are present in the bloodstream
of many Crohn's patients but no controls is Lancet 364: 1039, 2004.
I would ignore this -- Lancet has published too many bogus papers on GI pathology anyway.)
Claims from the early 1990's that
anti-mycobacterial therapy was very helpful in Crohn's didn't hold up.
One point against a link is that anti-TNF-α medications are notorious
for allowing ordinary TB![]() to disseminate; there has been no such
dissemination of mycobacteria in Crohn's patients treated with these drugs.
to disseminate; there has been no such
dissemination of mycobacteria in Crohn's patients treated with these drugs.
However, some problem with immune response to the normal gut flora is probably involved. Remember that the disease is usually worse in the terminal ileum (i.e., where the bugs really start to be numerous); there's also some experimental evidence including animal models.
Since giving an elemental diet helps (Dig. Dis. Sci. 42: 408, 1997; now mainstream), it's inviting to think that the local T-cells are angry with something in common food.
There is a familial tendency, with 37% concordance among identical twins. One susceptibility gene for familial's Crohn's has been located; NOD2/CARD15 (Gastroenterology 122: 867, 2002; Am. J. Gastro. 97: 3095, 2002; Lancet 359: 1661, 2002). This is some sort of an immune modulator, but exactly how it works is not clear.
Blacks seldom get Crohn's disease, while it is very common in some Jewish ethnic groups. The disease is more common in the developed world, and has been increasing considerably in frequency over the past few decades.
* Most interestingly, the more hygienic your parents kept their house, the more likely you are to get Crohn's (Lancet 343: 766, 1994).
Before relapses, mucosal levels of alpha-TNF and interleukin 1beta rise; watch for specific therapies directed against these (Lancet 353: 459, 1999).
* Smoking cessation greatly helps in the management of Crohn's: Dig. Dis. Sci. 57: 1026, 2012.
* One consistent finding in Crohn's is high level of SMAD7 protein, which inhibits TGF-beta-1 which is of course immunosuppressive. Oral mongersen, an antisense oligonucleotide, targets SMAD7 and seems to help Crohn's (NEJM 372: 1104, 2015).
Crohn's disease is a particular miserable one to have.
Patients are likely to suffer from a variety of systemic problems also seen in other kinds of inflammatory enteropathy. These include reactive arthritis ("enteropathic arthropathy"), uveitis, erythema nodosum, and (if HLA-B27 positive) reactive arthritis.
If you touch the bowel during surgery, a lesion will often develop at the site. Try not to operate on these people (though sometimes you must, for obstruction); the procedure is likely to make the process worse.
The monoclonals have revolutionized treatment of Crohn's.
* Ustekinumab, the anti-interleukin 12/23 monoclonal antibody, for Crohn's that does not respond to anti-TNF treatments: NEJM 367: 1519, 2012.
* Vedolizumab, the alpha4beta7 integrin antagonist, seems to work well: NEJM 369: 711, 2013.
In 1999, I predicted the remarkable responses to natalizumab ("Antegren", "Tysabri"), the α4 integrin inhibitor, for both ulcerative colitis and Crohn's (Gastroenterology 121: 268, 2001 and 122: 1592, 2002); NEJM 348: 24, 2003. The medication was withdrawn in February 2005 after two cases (only one tissue-confirmed) of progressive multifocal leukoencephalopathy but is now available again.
* The "holistic" lactobacillus therapy fails a scientific study miserably: Gut 55: 842, 2006. Omega-3's flop: JAMA 299: 1690, 2008.
* Future pathologists only: Obviously it's really important to distinguish TB granulomas and Crohn's granulomas in the gut. One group found all TB cases had CD73 staining of cells around the granuloma, and all Crohn's had none (Dig. Dis. Sci. 58: 2301, 2013).
* Dwight Eisenhower was operated for Crohn's during his presidency.
{09825} Crohn's disease, gross
{18707} Crohn's disease, gross
{19509} Crohn's disease, gross
{10190} Crohn's disease, histology
{10193} Crohn's disease, histology, with a granuloma
{20251} Crohn's disease, string sign
{20286} Crohn's disease, histology
{25464} Crohn's disease, histology
{26804} Crohn's disease, colon
MALABSORPTION is a common clinical problem.
 |
![]() Isospora
Isospora
Joel K. Greenson MD
U. of Michigan
Regardless of the cause, the effects of malabsorption are unpleasant.
Undigested food produces diarrhea. This is especially nasty when some substance is broken down into constituents but not absorbed (mucosal problems, disaccharidase deficiency).
If there is a shortage of bile, stools lack their normal brown color and look like clay instead. If there is malabsorption of fat ("STEATORRHEA"), stools are extra-stinky, greasy, and buoyant enough to resist flushing (late), and absorbing vitamins A, D, E, and K becomes a problem (early).
People with diseases involving the terminal ileum are prone to become deficient in B12 and folic acid. There may be loss of trace minerals. Much less well-known than vitamin deficiency is deficiency of trace metals. For example, lack of zinc produces skin problems like the genetic "acrodermatitis enteropathica".
"On the plus side" for most Americans, getting and staying trim is no longer a problem....
CELIAC SPRUE ("the most manageable autoimmune disease"; review from Mayo's: Arch. Path. Lab. Med. 134: 826, 2010; Am. J. Clin. Nutr. 69: 354, 1999; also NEJM 346: 180, 2002; Lancet 362: 383, 2003; Gastroenterology 128(S4: S-19 and S-74, 2005; Lancet 373: 1480, 2009; "keep the diagnostic criteria simple": Am. J. Med. 123: 691, 2010; either the serology or the biopsy should be acceptable for diagnosis Gastroent. 139: 12, 2010)
A very common disease caused by an idiosyncratic reaction to gliadin, a protein in the gluten of wheat, rye, and barley. (Oats are okay: Br. Med. J. 313: 1300, 1996; NEJM 337: 1884, 1997; still okay Dig. Dis. Sci. 51: 202, 2006).
The epitope is known (Nat. Med. 6: 337, 2000). Probably gliadin binds to the enterocyte, creating a hybrid antigen to which the immune system responds.
There's a lot of sprue around; don't hesitate to order your anti-tTG's / EmA. You have various tests to choose from and these will be different by the time you are in practice.
There are a few pitfalls -- for example, a patient who is IgA deficient may not make the IgA version of the antibody, so you check a total IgA as well, and/or order an IgG transglutaminase.
Transglutaminase is quite sensitive and fairly specific, though there's still plenty of people who you may want to do a duodenal biopsy on; in advanced sprue, flattening of the mucosa is obvious tp the endoscopist but it's a good idea to biopsy even if it looks normal; you may find the T-cells in the epithelium.
Today, the bloodwork is quite sensitive and specific for celiac disease (JAMA 303: 1738, 2010).
If the anti-tTG stuff comes back negative, and you're still thinking "celiac sprue", we may be forming antigen-antibody complexes in the gut itself, and your pathologist may be able to spot this (Gut 55: 1746, 2006). Mention the possibility. The pathologist might be able to do an anti-endomysial immunostain test. Update BMJ 334: 704, 2007.
The histology is typical. The epithelium on the villi fills with T-cells, and/or the villi shrink and then disappear along the small bowel, and the crypts deepen. Electron microscopists: The microvilli vanish, too.
The mature enterocytes are being destroyed by apoptosis (Am. J. Clin. Path. 115: 494, 2001), and the reserve cells are trying to replenish them. A pathologist will recognize increased mitotic activity in the crypts.
Not surprisingly, activated cytotoxic killer-T cells invade the epithelium itself (Am. J. Path. 148: 1351, 1996). Nowadays, this finding is key to the diagnosis, especially if the villi are not completely atrophic and/or the lymphocytes are abundant in the tips -- and remember the villi may even look normal in children with celiac sprue that's proven to be celiac sprue by a good response to gluten elimination (J. Ped. 157: 373, 2010).
I favor the Marsh grading / staging system (Gastrotenterology 102: 330, 1992):
Future pathologists: In the most severe disease, the villi are gone. If they are still there, you can still suggest a diagnosis of gluten enteropathy if the villi are obviously too short and the crypts are obviously hyperplastic.
Occasionally an identical histologic pattern appears as part of a self-limited illness with malabsorption ("probably a virus": J. Clin. Path. 121: 546, 2004).
Patients present with malabsorption, and an abnormally smooth gut mucosa (often lacking even the normal folds) is seen on endoscopy (Gut 31: 1080, 1988; NEJM 319: 741, 1988). The diagnosis is clinched when remission occurs following compliance with a gluten-free diet.
Around 10% of these people eventually get aggressive primary T-cell lymphoma (less often, carcinoma) of the gut if they're not properly treated.
Many of these patients also have "dermatitis herpetiformis", and conversely, most "dermatitis herpetiformis" patients have celiac disease, at least on biopsy.
 |
The "index patient" in Jerome Groopman's admittedly anecdote-based but disturbing
2007 best-seller was a woman with postprandial nausea and vomiting leading to
anemia, emaciation, and osteomalacia. Groopman reports she was assumed to have self-induced vomiting,
and visited around 30 physicians over around 15 years before a gastroenterologist drew blood and
endoscoped her and
made the easy diagnosis of celiac sprue. "A physician is only as a good as his/her index of suspicion." "Uncommon presentations of common diseases are more common than common manifestations of uncommon diseases." |
{15513} celiac sprue, small bowel; no villi
{19500} celiac sprue, small bowel; no villi
{19501} celiac sprue, small bowel; no villi
In TROPICAL SPRUE (Postgrad. Med. J. 82: 779, 2006), probably an infectious disease caused by one or more unknown bacteria, the crypts are hyperplastic, and the villi are usually short but seldom completely gone. (* Tip for future pathologists: Look for eosinophils!) These patients remit on long-term tetracycline, B12 and folic acid supplementation.
WHIPPLE'S DISEASE (Am. J. Surg. Path. 36: 1066, 2012)
Infection by Tropherhyma whippli bacillus (NEJM 327: 293, 1992; NEJM
332: 390, 1995), a close kin to the actinomyces![]() .
.
The bug has been observed for decades as PAS-positive rods inside histiocytes in the gut and elsewhere. Antibiotic treatment has long been known to eliminate the organism.
The disease is about twice as common in men as in women and predominantly in white people. No one knows why some folks can't shake this bug. In Whipple's disease, there doesn't seem to be any inflammatory response to the presence of millions of the little creatures.
It's a major mimic. Patients typically report having had "arthritis" for many years. In addition to malabsorption, the organism may involve lymph nodes (harmless), joints, endocardium (J. Inf. Dis. 190: 935, 2004) and/or brain (J. Neurosurg. 101: 336, 2004). Systemic Whipple's is easy to miss: Arch. Path. Lab. Med. 127: 1619, 2003; the harder you look, the more you find (Medicine 89: 337, 2010).
Once uniformly fatal, Whipple's disease is now easily treated with long-term antibiotic therapy. (* Tetracycline, nowadays trimethoprim-sulfamethoxazole Dig. Dis. Sci. 39: 1642, 1994 or new cephalosporins).
The bug was finally grown, in macrophage cell culture, in 1997. The trick is to add interleukin 4, which the bug evokes in vivo and which calms the macrophages (Lancet 350: 12262, 1997; more NEJM 342: 620, 2000; JAMA 285: 1039, 2001).
* The Whipple bacillus somehow suppresses the local immune system. When it is killed by antibiotics, a syndrome of "immune reconstitution" can occur and be quite serious (the body's angry with all the dead Whipple bugs, we can suppose -- Ann. Int. Med. 153: 710, 2010). You're familiar with this from AIDS as well, especially when there's cryptococcus on board in the CNS.
{06100} Whipple's disease
{06103} Whipple's disease, PAS
![]() Whipple's
Whipple's
PAS Stain
Wikimedia Commons
DISACCHARIDASE DEFICIENCY
Many adults lose their intestinal lactase (less often, other disaccharidases) as they get older. People of North European extraction tend to hold onto it longest; Blacks tend to lose it early. Rarely, the deficiency is present at birth.
Since lactose cannot be broken down, diarrhea results upon taking milk products.
Anyone who's recovering from any inflammatory disease of the gut is prone to be lactase deficient, at least temporarily.
If you are lactase deficient and still like your dairy foods, exogenous lactase (for your milk) and special ice cream are available. Mmm.
* Future researchers: The normal gut flora breaks lactose down into products including hydrogen, so some people make the diagnosis by measuring breath hydrogen. (No, this isn't bad enough to cause problems at birthday parties....) I suggest taking a history and making a therapeutic trial instead.
* The catastrophic autosomal recessive "microvillous inclusion disease" produces near-absent microvilli and villi; it's a pediatric nightmare. Let us worry about it.
ABETALIPOPROTEINEMIA (J. Clin. Inv. 120: 2889, 2010)
Difficulty making apolipoprotein B48 and B100, which is necessary to absorb fat. Patients also lack chylomicrons, VLDL's, LDL's, and have scrambled lipid content in cell membranes (look for "spiny red cells", or "acanthocytes" / "E-T finger cells"; distinguish them from "echinocytes" which have evenly-spaced spicules). Pathologists see enterocytes loaded with dietary fat that has nowhere to go. Rare, but tends to pop up on exams because we understand the molecular biology. Mild cases might be "longevity genes" and a reason for some people just having low LDL's.
INTESTINAL OBSTRUCTION
One of the most unpleasant, slowest ways to die. There are a variety of causes.
You may hear of the non-mechanical problems being called "paralytic ileus". Unless the bowel is paralyzed, obstruction produces severe crampy-colicky pain.
HERNIAS result when gut enters a defect in the wall of the peritoneal cavity. Most often, this is in a man's inguinal ring, though there are a variety of other possible locations.
ADHESIONS are fibrous bands that follow peritonitis from any cause (most typically, peritoneal irritation during surgery). These can snare loops of bowel and require re-entry into the abdomen.
{40680} adhesions
{40681} adhesions
INTUSSUSCEPTION is a telescoping of the bowel into itself, often because of a bump in the wall (big Peyer's patch, polyp, Meckel's) and the gut mistakes it for dinner.
Most common in kids, you can see it at any age. Future radiologists: Here's one you can sometimes both diagnose and cure with a barium enema!
* Philologists: The trapped part is the "intussusceptum". The enclosing part is the "intussuscipiens".
* The hoopla over the original rotavirus vaccine was that it might cause a few cases of intussusception -- as a result, it was banned in the USA and made unavailable for the millions of poor kids overseas at risk for dying of rotavirus. Today's rotavirus vaccine does not cause a measurable risk for intussusception (JAMA 307: 598, 2012).
{09832} intussusception
{38677} intussusception, colonic, with gangrene
{39391} intussusception
VOLVULUS: Twisting of a loop of bowel 360 degrees around its stalk (or Meckel's). Rare, but don't miss it. When it occurs in the colon (most often sigmoid, but anyplace is possible), the lowest-level medical student is given the privilege of untwisting it, while everyone else stands way back (why?)
{07210} volvulus
{24441} meconium ileus and volvulus (cystic fibrosis)
{46271} volvulus, sigmoid colon ("chronic")
CARCINOID TUMORS (low-grade, low-aggressiveness "neuroendocrine tumors"): Cancers arising from the endocrine (paracrine, Kulchitsky, enterochromaffin, APUD, neuroendocrine, neurosecretory, chromaffin, etc., etc.) cells of the gut or elsewhere. Most look and act relatively non-aggressive, but they are often discovered only when metastatic disease has already appeared. Reviews Lancet 352: 352, 1998; NEJM 340: 858, 1999; Gastroent. 128: 1717, 2005; Am. Fam. Phys. 74: 429, 2006.
The cells are cuboidal and monotonous, and the architecture is is often like simple shapes from geometry / an arabesque. Depending on the site, carcinoids tend to secrete various hormones (check "Big Robbins" for the list, which is long).
You'll see neurosecretory granules, if you stain for them or use EM. As you know, they'll be at the bottoms of cells (in the non-neoplsatic counterparts, this is where they synapse with the nerve twigs). Synaptophysin is a good stain to use to see them; it helps make the call.
Carcinoids are very common in the appendix (1 in 300 autopsies). Here, and in the rectum, they have only limited ability to metastasize.
Carcinoids elsewhere may be more aggressive.
* The molecular biology is only now starting to be worked out. There seems to be no trademark mutation yet (Cancer 109: 2420, 2007); the little that's known does not support the WHO's idea that carcinoids and islet cell tumors should be classified together as "gastroenteropancreatic neuroendocrine tumors" (Cancer 104: 2292, 2005; this isn't going to affect clinical care in any case).
When the liver cannot detoxify the secretory products of the carcinoid (i.e., it is not in the portal system, or there are liver metastases), patients are prone to symptoms.
The classic carcinoid syndrome (blamed in part on serotonin) involves (1) wheezing; (2) flushing; (3) fibrosis of the right-sided endocardium (lung detoxifies whatever does this).
* The truth is that nobody knows which tumor product causes the fibrosis of the right-sided endocardium, though serotonin is once again a "usual suspect".
Prolonged survival is common in carcinoid disease, even with liver metastases. (Surgeons: You may de-bulk them -- and this helps; see Arch. Surg. 141: 1000, 2006; arterial embolization often helps as well Cancer 104: 1590, 2005.)
Future clinicians: Suspecting a carcinoid? Check the urine for the serotonin metabolite, 5-HIAA (5-hydroxy-indole-acetic acid). Even better... if you really think this might be carcinoid, an isotope scan using 111-In-pentetreotide (an octreotide analogue) will light up carcinoids (good for other neuroendocrine tumors too; in high doses it can used for radiotherapy).
* The best screen may be blood chromogranin A (Ann. Surg. 243: 273, 2006). Several circulating tumor markers are known including chromogranin A (Cancer 10: 459, 2003). Watch blood neurokinin A as a marker for carcinoid, especially as a marker for its continued presence after resection / responsiveness to octreotide therapy (Gut 55: 1581, 2006).
{19521} carcinoid, appendix, gross
{19522} carcinoid, appendix, gross
{19508} carcinoid, small bowel, histology
{49187} carcinoids, small bowel, gross
{24678} carcinoid, small intestine
{26348} carcinoid, ileum
{09175} carcinoid, electron micrograph
{09176} carcinoid, electron micrograph
Future pathologists mostly:
* ARGENTAFFIN: Capable of reducing silver (and thus having the granules stain black) without a separate reducing agent.
* ARGYROPHIL: Capable of reducing silver (and thus having the granules stain black) so long as a separate reducing agent is supplied. All argentaffin cells are also argyrophil.
CHROMOGRANIN, now a tumor marker in clinical use, is a classic immunostain for carcinoid, adrenal medulla, and generally for "neuroendocrine" stuff. SYNAPTOPHYSIN is also in widespread use to confirm that a GI tumor is carcinoid or at least shows "neuroendocrine differentiation."
* Foregut carcinoids are almost never argyrophil. (NOTE: This includes lung, duodenal, and biliary carcinoids. These are not usually serotonin / "carcinoid syndrome" producers, but might make something else.) All about gastric carcinoids: Cancer 73: 2053, 1994.
* Midgut carcinoids are almost always argyrophil. (NOTE: This includes small intestinal, appendiceal, and most colonic carcinoids. These are usually hormonally active.)
* Hindgut carcinoids are variable. (NOTE: Descending colon and rectum.) They seldom produce carcinoid syndrome.
* Leave the diagnosis of lymphomas of the midgut and hindgut to us. "Lymphomatoid polyposis" is multifocal mantle cell lymphoma, often around the ileocecal valve.
* "Autistic enterocolitis" does not exist. This was invented by Andrew Wakefield, the principal instigator of the MMR-and-autism fraud while he was secretly receiving large amounts of money from anti-immunization tort lawyers. The original article described normal histology, which the author called abnormal, and somehow this got past the editors. This was noted by your lecturer; Lancet declined to publish my letter to this effect. However, the rest of the pathology community agrees with me (Histopathology 50: 371, 2007). In 2011, it was revealed that the biopsies had been read as normal or near-normal by the pathologists, and that Wakefield had re-diagnosed them as abnormal. There is nothing "spiritual" about "keeping an open mind" about this crime against humankind, which has cost more than a few children their lives and greatly interfered with your ability to keep the public safe.
Small bowel biopsy can be performed using standard endoscopy, or a swallowed device ("Watson capsule", "Storz capsule") that is monitored on fluoroscopy and then retrieved (Scand. J. Gastro. 36: 1230, 2001). "Wireless capsule endoscopy" is an exciting new technology. The patient swallows a capsule containing a tiny video camera, a transmitter, and an antenna. Using it to confirm the diagnosis of Crohn's: Gut 52: 390, 2003.
|
 |
|
APPENDIX |
|
There's less "mystery" to our having the appendix than "Big Robbins" would have you believe. Many animals have a large pouch here that they need for digestion. We've still got it, but it's not an obvious asset. (* Darwin's world; the imperfections of nature tell stories of our origins. Pseudoscience fans: Ignore what you've heard about the appendix being essential for the developing immunity of the unborn child. It's only one of many sites where B-cells can mature). It's also handy for us in this day of modern antibiotics -- perhaps it's a reservoir for the "nice" bacteria which can repopulate the gut. I look forward to a study showing that people who have had appendectomies do worse after bacterial colon infections generally.
A familiar, common surgical problem, mostly of young people, caused (in most cases, we think) by obstruction of the lumen (usually a fecalith or hyperplastic lymphoid tissue, less often a tumor, gallstone, or maybe pinworms).
Probably impaction by a fecalith is most important, since appendicitis is rare in countries with high-bulk eating habits.
In folks older than 30 with acute appendicitis, about 10% have obstruction by a serrated adenoma, far more than random. You do have to look thoroughly (Am. J. Clin. Path. 126: 875, 2006).
* The bacteria that usually infect the tissue are usually the ubiquitous fusobacteria that inhabit the gut (Gut 60: 34, 2011).
* The neurons in an acutely-inflamed appendix are likely to be hypertrophied, indicating that there's been obstruction for a long time before things got really nasty (Arch. Path. Lab. Med. 124: 1429, 2000).
Measles![]() was once famous for causing appendicitis that exhibits the
classic Warthin-Finkeldey giant cells. Two cases from contemporary South Korea:
Arch. Path. Lab. Med. 126: 82, 2002.
was once famous for causing appendicitis that exhibits the
classic Warthin-Finkeldey giant cells. Two cases from contemporary South Korea:
Arch. Path. Lab. Med. 126: 82, 2002.
{20088} appendicitis with fecalith
![]() Appendix pinworms
Appendix pinworms
Wikimedia Commons
As mucus continues to be secreted behind the obstruction, the pressure builds, the epithelial barrier breaks, the bacteria can penetrate the wall, and true infection quickly begins.
As the osmotic pressure within the pus builds up to tremendous levels, the appendix becomes gangrenous (vascular compromise) and/or bursts (nasty, you'll get peritonitis or worse).
Early symptoms are a poorly-defined belly-ache (typically referred to the umbilicus) and no appetite ("Would you like some ice cream?" "NO!!"), with maybe fever and leukocytosis. Later, when the appendix presses against peritoneum, the pain becomes knife-like and peritoneal signs appear. Call a surgeon.
Surgery's still best once appendicitis is proven on CT scan. "Give them antibiotics and watch them" is the other idea, even with today's super-meds, the outcome's not so good (JAMA 313: 2340, 2015).
The pathology is what you'd expect. Early, there's the obvious hyperemia. Later, there's fibrin on the outside, pus on the inside. At the end, there's gangrene. Again, the weakened wall may rupture, spreading the infection.
{13283} acute appendicitis, gross
{10196} acute appendicitis, gross
{11445} acute appendicitis, gross
{19526} acute appendicitis, histology
{17558} acute appendicitis, histology
{17562} acute appendicitis, polys
|
Australian Pathology Museum High-tech gross photos
|
|
|
Future surgeons: If fewer than 20% of your operations for "appendicitis" don't reveal a normal appendix, your index of suspicion is low. Once in there, you may find mesenteric adenitis (Yersinia enterocolitica or Yersinia enterocolitica), an inflamed Meckel's, the GI 'flu, gonococcal salpingitis, etc., etc.
Your lecturer predicts that surgery will remain standard treatment as soon as the diagnosis is made, and that the "antibiotics first" strategy will prove more pricey and have poorer outcomes (NEJM 372: 1937, 2015).
GRANULOMATOUS APPENDICITIS, which looks histologically like Crohn's but is limited to the appendix, has a benign follow-up (J. Am. Coll. Surg. 185: 13, 1997).
* I got a chuckle from a surgeon's claim (Lancet 347: 1076, 1996) that a "histologically normal appendix" removed at surgery for suspected appendicitis often exhibits widespread immune activation. The "immune activation" looks like the result of overstaining the sections.
MUCOCELE of the appendix is an appendix transformed into a bloated, tense-walled bag of mucus.
The cause may be (1) a hyperplastic / serrated polyp of the appendix; (2) a mucin-producing adenoma; (3) a mucinous cystadenocarcinoma.
Of these:
CARCINOID is the common tumor of the appendix. It is a very low-grade malignancy.
* There are two varieties: Arch. Path. Lab. Med. 134: 871, 2010 -- pure carcinoids, and those that also produce mucin ("goblet cell carcinoids"). Common carcinoid generally has a good prognosis, but if the pathologist finds a goblet cell carcinoid, it's good to do a right hemicolectomy after. Attempts by pathologists to tell the bad-acting goblet cell carcinoids from ones that might be tamer have not been successful: Am. J. Surg. 202: 400, 2011.
COLON AND RECTUM
 Colon Exhibit
|
|
{49202} melanosis coli from cascara laxatives, the terminal ileum is normal color
![]() Lymphocytic colitis
Lymphocytic colitis
Joel K. Greenson MD
U. of Michigan
Terms:
TENESMUS is the continuous, painful urge to defecate, whether or not you really need to do so. Any inflammatory problem in the anus or rectum is likely to lead to tenesmus, which is very unpleasant.
DYSENTERY is the passage of bloody-mucoid stools, usually not voluminous, usually painful.
Worth knowing: Bloody diarrhea is almost always due either to inflammatory bowel disease (ulcerative colitis, Crohn's -- you will see distorted architecture on biospy), or bad infection (shigella, bad E. coli, amoebas -- you probably won't see distorted architecture on biopsy, apart from maybe ulcers), or ischemic colitis (atrophic glands in a hyalinized lamina propria.)
BIRTH DEFECTS
MALROTATION may first become apparent when the inflamed appendix isn't where it should be. REDUPLICATION may produce double-barreled portions of the colon or rectum. One kid in 5000 has an IMPERFORATE ANUS (failure of the cloacal diaphragm to open; there are several varieties, including those with fistulas to nearby organs).
{49199} imperforate anus ("atresia of the anus")
* There are normally some white cells (mostly lymphocytes, plasma cells, and some eosinophils) in the colonic mucosa, but they are not so numerous as in the small bowel, and if they extend all the way to the muscularis mucosae, there is probably some real inflammation here.
* ACUTE TYPHLITIS today describes bacterial ulcers of the cecum, a potentially deadly hazard in those who lack neutrophils. Update Cancer 104: 380, 2005.
DIVERSION COLITIS ("pouchitis") results from depriving mucosal cells of the bacterially-produced short-chain fatty acids they use as their primary nutrient. This can happen when a diverting colostomy is performed proximal to a portion of bowel; we treat it with fatty acid enemas. The histology is nonspecific, with goblet cell depletion, inflammation, maybe crypt abscesses, often prominent germinal follicles. The same mechanism is seen in starvation colitis (Lancet 385: 1696, 2015.)
* "Chronic active colitis" is a nonspecific, uncommon term used when there are some crypt abscesses and apoptotic epithelial cells. There may also be granulomas, as in the most recently discovered cause -- cord-blood stem-cell transplantation (NEJM 365: 815, 2011).
HIRSCHSPRUNG'S DISEASE ("congenital megacolon"; Am. Fam. Phys. 74: 1319, 2006; seven consonants in a row) results from failure of Auerbach's and Meissner's plexuses to develop over a stretch of bowel, usually rectosigmoid. If the entire colon is involved, it's AGANGLIONOSIS; otherwise, the disease can be treated successfully by removing the aganglionic segment.
This isn't rare. Around 1 in 6000 people suffer from Hirschsprung's.
Every once in a while, it develops in an older child or adult.
Future pathologists: You will make the diagnosis on RECTAL SUCTION BIOPSY, which samples the mucosa without any need to get the ganglion cell layer itself. In the absence of proper ganglia, the unmyelinated cholineregic nerve fibers in the mucosa and submucosa are thicker and more abundant (Arch. Path. Lab. Med. 122: 721, 1998), and distinguishing this from normal is usually easy. We see them best with acetylcholinesterase staining.
* Future pathologists: An adequate biopsy has to have a fair amount of submucosa. If you only have muscularis mucosae, try a calretinin stain -- positive fibers in the lamina propria say "no Hirschsprung's"; absence of positive fibers in the lamina propria say "Hirschsprung's". Arch. Path. Lab. Med. 137: 1099, 2013.
{20090} aganglionic megacolon
* The first Hirschsprung's gene turned out to be an allele at the RET receptor (MEN-IIb locus, for GI tract ganglioneuromas.) See Nature 367: 319, 1994; good RET product seems to be required to prevent apoptosis of neurons, at least in an animal model (J. Clin. Inv. 118: 1890, 2008). More recently, both endothelin 3 and endothelin receptor have proved to be Hirschsprung loci.
* INTESTINAL NEURONAL DYSPLASIA is a Hirschsprung's variant with an okay Auerbach's plexus but lots of giant ganglia in the submucosa instead of the hypertrophic nerve trunks and excessive adrenergic and cholinergic fibers seen in the submucosa in Hirschsprung's. See Gut 48: 671, 2001. Slow-transit chronic constipation ("colonic inertia") might perhaps be a forme fruste of IND, with malformations of the ganglionic plexus. One report: Eur. J. Gastro. 12: 755, 2000.
For an adult, there are many causes of megacolon, including damage to the nerve tissues from inflammatory disease. Pretty much the only thing that selectively destroys ganglion cells is Chagas' disease.
{49197} acquired megacolon
DIVERTICULAR DISEASE ("ticks")
This common problem is the result of the mucosa pooching out through the weak spots where vessels penetrate the muscularis propria 120 degrees on either side of the mesentery.
At least a few diverticula are present in most older people eating a "western diet". The cause, of course, is high intra-lumenal pressures necessary to propel these peoples' hard little feces. As you would expect from the etiology, diverticula are most numerous distally.
Purists: Of course, these are really "pseudo-diverticula".
Usually asymptomatic (the bowel complaints are a result of the high intraluminal pressures), uncomplicated DIVERTICULOSIS (maybe we should just call it diverticular disease) may result in copious bleeding if a feeder artery gets nicked.
{42227} colonic diverticulosis, gross (inflated specimen)
{08086} colonic diverticulum, histology (this is all
mucosa, protruding out into adventitia)
{10514} colonic diverticulum with bleeding point
{19702} diverticulosis coli, x-ray
{24425} diverticulosis coli, x-ray
{39995} diverticulosis; barium fills the "ticks"
DIVERTICULITIS ("left-sided appendicitis") results from one diverticulum getting infected, probably when a fecalith occludes its mouth and lets bacteria proliferate.
Suppuration may result, and nearby diverticula may become involved when bacteria spread and edema narrows their mouths.
The process usually subsides, but surgery may be required. Severe diverticulitis may cause scarring and chronic problems.
ISCHEMIC COLITIS causes bleeding in patients with vascular or cardiac insufficiency when the mucosa (usually at the splenic flexure and/or rectosigmoid) undergoes necrosis. Pathologists look for atrophic glands in a densely-collagenized lamina propria -- this establishes the diagnosis of ischemic colitis but not the exact cause.
FUNCTIONAL BOWEL SYNDROME ("spastic colon") is cramping, constipation, and/or diarrhea without a good anatomic correlate.
Long attributed to "emotional causes", and then to "inadequate fiber in the diet", at least part of the problem is uncoordinated peristalsis, resulting in a portion of the bowel trying to push feces through a distal portion that is clamped shut ("segmentation"). (This may also be a mechanism underlying diverticular disease.)
Probably the gut flora plays a role as well, since rifaximin seems to help (NEJM 364: 22, 2011).
* The most interesting work on "functional" bowel syndrome (now obviously a misnomer) is on mast cells that degranulate too readily. Excellent results are coming from use of a systemic mast-cell stabilizer (Gut 59: 1213, 2010).
* "The mind and the gut": The "emotional causes" business may reflect the common experience that anxiety speeds transit time, and depression slows it; some enterprising psychiatrists actually quantitated this in 1996, and found that anxious psych patients averaged a 14 hour transit time, depressed psych patients averaged a 49 hour transit time, and controls averaged a 42 hour transit time (Br. Med. J. 1996).
* Future pathologists: Ignore anything anybody tells you about determining post-mortem interval from how far dinner (eaten at a known time) has passed along the gut.
* Amoebas probably are not an important cause of functional bowl syndrome symptoms (Lancet 349: 89, 1997).
* Type 3 serotonin receptor blocker (alosetron) for spastic colon: Lancet 355: 1035, 2000. The medicine was approved too fast and killed people by producing ischemic colitis: Lancet 357: 1544, 2001. It's now back, but be careful.
HEMORRHOIDS are dilated perianal venous plexi.
The causes are (1) constipation and straining at stool; (2) venous stasis of pregnancy; (3) portal hypertension.
Rectal problems attributed to hemorrhoids may simply be due to constipation. However, a
thrombosed or twisted-infarcted hemorrhoid can be very painful. Bleeding hemorrhoids in portal
hypertension can be fatal (Dr. Livingstone, of "I presume" fame, died this way; he may have had
portal hypertension due to schistosomiasis![]() ).
).
|
|
ANGIODYSPLASIA of the colon is a dilatation of vessels, usually in the cecum of older people, that can bleed slowly or copiously.
Angiographers see this lesion more readily than do pathologists, since the lesion collapses on removal from the body.
It's a famous and common cause of iron-deficiency.
|
|
{08088} angiodysplasia of cecum; the glands are normal
INFECTIOUS COLITIS
In the unlikely event that this is biopsied, the pathologist will see neutrophils in the epithelium and lamina propria. The glands will not be disrupted, and there will not be plasma cells; the absence of plasma cells is very helpful in being sure this is not ulcerative colitis.
IDIOPATHIC ULCERATIVE COLITIS (Lancet 359: 331, 2002; NEJM 365: 1713, 2011).
|
|
|
|
|
|
|
|
An inflammatory disease of unknown etiology but predictable pathology. It affects around 1 person in 1000.
The disease begins in the rectum and may extend up as far as the cecum. The pathology is continuous, without the "skip lesions" of Crohn's. (* Well, sometimes it's patchy, but usually it's continuous up from the rectum. Am. J. Gastro. 92: 1247, 1997; J. Clin. Path. 49: 319, 1997.)
Involvement of the terminal ileum is called "backwash ileitis" (review for pathologists, with criteria: Am. J. Clin. Path. 126: 365, 2006; focus on how to tell it from Crohn's; not surprisingly, backwash ileitis is continuous and confined to the mucosa). Otherwise, the small bowel is spared.
There may be systemic problems, most notably enteropathic arthritis, erythema multiforme, and uveitis, as well as sclerosing cholangitis and even the dread, necrotizing skin lesion "pyoderma gangrenosum".
* An interesting finding is that, if your assay is super-sensitive, a large majority of ulcerative colitis and/or primary sclerosing cholangitis patients have small amounts of anti-neutrophil cytoplasmic antibodies on board (Am. J. Clin. Path. 99: 277, 1993). These antibodies seem to be directed against lactoferrin, cathepsin, lysozyme, and/or beta-glucuronidase, but not proteinase 3 (Wegener autoantigen) or myeloperoxidase (polyarteritis autoantigen). Look at the photos in Dig. Dis. Sci. 55: 733, 2010 and tell me whether you saw vasculitis as a principal problem like the authors did.
The pathology is inflammation (predominantly plasmacytic), hemorrhage and tissue loss. Except in the most severe cases, the damage is strictly limited to the mucosa.
Look for "crypt abscesses", accumulations of neutrophils in the dilated bases of surviving colonic crypts. These are fun to find, and are usually abundant in ulcerative colitis, but not pathognomonic of anything.
As the ulcers coalesce, the surviving mucosa sticks up as PSEUDOPOLYP. These may grow long and look like worms. Or they may tunnel under a "bridge" of intact mucosa.
In the most severe cases (as with any severe, extensive inflammatory colonic disease), "toxic megacolon" may develop, with the bowel wall paralyzed and the lumen filled with incredibly nasty stuff. Call a surgeon to perform a total colectomy.
In milder cases, lesions in various stages of healing are common.
![]() Ulcerative colitis, acute lesions
Ulcerative colitis, acute lesions
Classic drawing
Adami & McCrae, 1914
The cause remains obscure.
By now, there is a consensus that the disease is caused by some immune reaction between the gut mucosa and the contents of the large intestine. Beyond this, there's still no unifying a large number of observations (Lancet 369: 1025, 2007).
It's easiest to think that some bacterial product in the gut of specially-vulnerable people damages the colonic epithelium, shutting down metabolism of fatty acids (Gut 35: 73, 1994; Lancet 343: 35, 1994). The best candidate right now is a fusobacterium that produces butyric acid (Gut 52: 79, 2003). The abundance of bacteria in the crypt mucus before the gut breaks down is well-known to pathologists and can now be quatitated without biopsy (Ann. Surg. 252: 869, 2010.
Or perhaps it's the immune response to the product of some bacterium. One interesting claim is that administration of the "kinder, gentler" colon bacterium Bifidobacterium longum brings about impressive relief (Gut 54: 242, 2005). Stay tuned.
* Isotretinoin ("Accutane") alters epithelium, and seems to exacerbate ulcerative colitis and Crohn's disease (Gut 58: 737, 2009). This is presently being litigated in the USA.
Whatever the cause, the disease is supposed increasing in prevalence in the U.S.; I suspect the diagnosis is simply made more often. The disease waxes and wanes, though the talk about "stress" as a precipitator hasn't held up.
* The 1997 media hoopla about measles![]() vaccine causing ulcerative colitis
(refuted): Lancet 350: 764, 1997. The author of the original
article was none other than the convicted fraud Andrew Wakefield (Gastroent. 108: 991, 1995.)
vaccine causing ulcerative colitis
(refuted): Lancet 350: 764, 1997. The author of the original
article was none other than the convicted fraud Andrew Wakefield (Gastroent. 108: 991, 1995.)
As you would expect, patients are troubled with bloody diarrhea, and may have systemic symptoms. The most serious complication is the development of adenocarcinoma of the colon.
Gastroenterologists follow patients with this disease, and if the mucosal cells begin to look dysplastic, colectomy is probably advisable (Lancet 343: 71, 1994). If the crypts are involved but the surface spared, the pathologist is required to call "indefinite for dysplasia." The cancer risk continues even when the disease is quiescent (Gastroent. 103: 431, 1992), and historically was said to approach 100% in thirty years. Thankfully, this is no longer the case.
* A group at Stanford has a fluorescent protein for use during endoscopy that binds selectively to dysplastic epithelium. Watch this one: Nat. Med. 14: 454, 2008.
The worse the ongoing inflammation, the greater the cancer risk (Gastroent. 133: 1099, 2007). But all these patients need to be under care, and for this you need your pathologist.
Today's risks for cancer in all patients, without regard to histology, are 2% at 10 years, 8% at 20 years, and 18% at 30 years (Br. J. Surg. 92: 928, 2005). If active surveillance reduces the risk, it has resisted demonstration (J. Thorac. Card. Surg. 146: 365, 2013).
Dysplasia is recognized as hyperchromatic nuclei, and scored as low- or high-grade primarily based on whether the nuclei are lined up evenly or not.
Nobody really knows the risks, though pathologists do feel comfortable making these calls (Arch. Path. Lab. Med. 137: 338, 2013). High-grade dysplasia calls for colectomy. Right now, a pathologist's call of "low grade dysplasia in the crypts" probably does not justify colectomy, and pathologists can't agree among ourselves whether it is present in particular specimens: Gut 52: 1127, 2003. But "low grade dysplasia on flat epithelium", has a 50% chance of going malignant in five years (Gastroenterology 125: 1311, 2003).
* This is an exciting time for the medical therapy of ulcerative colitis. You'll learn about this, and the colorectal cancer surveillance that these folks (and Crohn's folks) require, on rotations (review NEJM 372: 1441, 2015). If the sulfa and the steroid enemas fail, and you elect "no surgery", consider cyclosporine by vein (NEJM 330: 1841, 1996). Newer remedies include epidermal growth factor per rectum (NEJM 349: 350, 2003), infliximab (Gastroent. 128: 1805, 2005; the anti-TNF agent golimumab for months of control with one injection Gastroent. 146: 85, 2014. Gastroenterology 141:1194, 2011), rebamipide enemas (Dig. Dis. Sci. 50 S1: S-119, 2005), and the anti-CD3 monoclonal antibody visilizumab (Gastroent. 133: 1414, 2007), and rosiglitazone (Gastroenterology 134: 688, 2008). Vedolizumab, the alpha7beta4 integrin antagonist: NEJM 369: 699, 2013. Etrolizumab, an antibody against an adhesion molecule component: Gastroenterology 146: 307, 2014. There are others underway. A more mundane approach may simply involve giving oral phosphatidylcholine (Ann. Int. Med. 147: 603, 2007).
Removal of the colon at any time cures ulcerative colitis.
Future clinicians beware: Shigellosis and amebiasis can mimic ulcerative colitis pretty well. Future pathologists:
|
|
Here is the inevitable chart comparing "Crohn's" and "Ulcerative Colitis"...
| CROHN'S DISEASE | ULCERATIVE COLITIS | |
| Etiology? | Unknown / immune? | Unknown / immune? |
| Sex? | equal | slightly more among females; |
| Ethnic group? | more among Jewish | more among Jewish |
| Hereditary? | Contributes | Contributes |
| Exacerbate/remit? | Yes | Yes |
| Stress exacerbates? | Maybe | Maybe |
| Smoking? | Makes worse, try to quit | Quitting may exacerbate |
| Location? | Variable | Rectum and upwards |
| Bowel? | Small more than Large | Large only |
| Terminal ileum? | Favorite site | "Backwash" |
| Colon? | Right more than left, if any | Left more than right |
| Bile ducts? | May be damaged (Crohn's itself) | May be damaged (sclerosing cholangitis) |
| Anal troubles? | Common | No |
| Oral lesions? | Maybe | No |
| Skip lesions? | Yes | No; continuous |
| Layers? | All three | Mucosa only |
| Ulcers? | Linear fissures | Broad / irregular |
| Pseudopolyps? | May be some | Usually, may be spectacular |
| Fibrosis? | Severe | No |
| Fistulas? | Yes | No |
| Creeping fat? | Yes | No |
| Granulomas? | Often | No |
| Bleeding? | Subtle | Heavy-duty |
| Pain? | Wretched | Not so much |
| Malabsorption? | Maybe | No |
| Bowel obstruction? | Maybe | No |
| B-12 deficiency? | Maybe | No |
| Lymphs/plasma cells? | Yes | Yes |
| Arthritis, uveitis? | Yes | Yes |
| Ankylosing spondylitis? | if (+) for HLA-B27 | if (+) for HLA-B27 |
| Diagnosis? | Tough | Easy |
| Surgery? | Avoid | Cures |
| Carcinoma risk? | Fairly low | High in the long run |
PSEUDOMEMBRANOUS COLITIS: Clostridium difficile overgrowth, usually because of previous antibiotic use. Very common. Classic review: NEJM 334: 257, 1994.
Remember the ileum can be involved as well as the colon, and can even perforate (Arch. Surg. 141: 97, 2006).
The new DNA amplification test seems to be the best (Dig. Dis. Sci. 57: 2592, 2012).
* Duodenal infusion of donor feces for recurrent pseudomembranous colitis: NEJM 368: 407, 2013. "Much better than vancomycin." If you say so. The conquest of pseudomembranous enterocolitis may be here with administration of spores of nontoxigenic C. difficilemicrobse strain M3 (JAMA 313: 1719, 2015).
![]() Pseudomembranous colitis
Pseudomembranous colitis
Patches of pseudomembrane
KU Collection
![]() Pseudomembranous colitis
Pseudomembranous colitis
Great photos
Pittsburgh Pathology Cases
HEMORRHAGIC ENTERCOLITIS is another antibiotic-induced illness, this time with hemorrhage rather than with a pseudomembrane. The etiologic agent appears to be cytotoxin-producing Klebsiella oxytoca (NEJM 355: 2418, 2006).
(NEONATAL) NECROTIZING ENTEROCOLITIS (Lancet 368: 1271, 2006)
A serious gut problem in babies, especially bottle-fed preemies who have received indomethacin and dexamethasone (Pediatrics 119: e164, 2007). The etiology is unclear but is probably infectious.
Inflammation and necrosis of the terminal ileum, cecum, and ascending colon produce a medical and surgical emergency.
Clearly multifactorial (gut contents, prematurity, lack of oxygen to the gut, who knows what else?), the disease seems to be less common if probiotics ("nice germs") are administered (Lancet 369: 1614, 2007).
LYMPHOCYTIC COLITIS is said to present when a patient has watery diarrhea and 20 or more lymphocytes in the epithelium for every hundred epithelial cells. Mostly a disease / reaction pattern in older women.
COLLAGENOUS COLITIS (see Gut 44: 881, 1999; histopathology Am. J. Gastro. 98: 340, 2003; Arch. Path. Lab. Med. 134: 1483, 2010)
A newly-recognized illness of older adults (mostly women) featuring a dense band of collagen under the surface mucosa of the colon. (* Ten or more microns thick.)
The etiology is obscure, but patients often have evidence of autoimmunity. The collagenous band is often accompanied by a chronic inflammatory infiltrate, including lymphocytes in the epithelium. (The cases I've seen remind me of the infiltrate you see in active scleroderma.)
Patients have difficulty absorbing water and electrolytes from the colonic contents. It would seem reasonable that the collagenous band simply interferes with their reabsorption.
Future endoscopy artists: The colon may look normal. Biopsy anyway. Future pathologists: Beware, a collagenous band can be seen in ulcerative colitis and in Crohn's.
* Apparently NSAIDS can cause these people to get superimposed ulcers: Am. J. Gastro. 98: 1834, 2003.
{08103} collagenous colitis (thin band under
the surface mucosa; the normal colonic glands are cut at an angle)
{08104} collagenous colitis
![]() Collagenous colitis
Collagenous colitis
Joel K. Greenson MD
U. of Michigan
* A similar lesion in the small bowel is an uncommon cause of malabsorption ("collagenous sprue"; Arch. Path. Lab. Med. 135: 803, 2011).
FECAL IMPACTION (J. Clin. Gastro. 30: 228 & 331, 2000; "the condition we don't discuss": JAMA 285: 1265, 2001)
A rectum (usual location) full of hard, immobile feces. No joke. And often missed. You'll learn the techniques of "rapid digitalization" and "3H enema" ("high, hot, heck-of-a-lot") to remove these in the clinic.
An under-recognized lesion is "stercoraceous ulcers" (stercoral ulcers), pressure decubiti from fecal impaction. A common autopsy finding in hospitals where bowel care is sometimes neglected, and an entry route for "idiopathic sepsis". See South. Med. J. 99: 521 & 525, 2006 for a description of a situation that must be common.
BENIGN COLON POLYPS 
Today, nobody seriously questions that even the banal hyperplastic polyps are true neoplasms resulting from mutations of genes (known and probably unknown) related to real colorectal cancer. Most benign colon polyps are either pedunculated (on a stalk) or sessile (slightly elevated). A few may are flat and even fewer are depressed.
HYPERPLASTIC POLYPS are the most common lumps and bumps in the colon. Most older people have some.
Grossly, they usually look like rice grains on the colonic mucosa. These tiny things are easily recognized by colonoscopists and do not get biopsied.
Histologically, they look like colonic mucosa with cells of variable height in the crypts creating a distinctive scalloped appearance.
* Pathologists have tried subclassifying these based on how much mucus is produced; the genetics varies but it doesn't seem to matter.
The significance of a real hyperplastic polyp to a person's health is zero, not even an indication for more frequent colonoscopy.
* People who have actually looked have found mutated BRAF and/or mutated KRAS in many but by no means all of these little things.
{15516} hyperplastic colon polyp, histology
{15517} hyperplastic colon polyp, histology
* Future pathologists only: The dysplasia is thought to indicate that abnormal methylation has begun. It can be either the conventional dysplasia seen in tubular and villous adenomas (purple-staining, very skinny "pencil" cells) or "serrated dysplasia" (pink-staining cuboidal cells with prominent nucleoli).
Some new accounts claim that up to 10% of colonoscopies detect at least one sessile serrated adenoma (Gastroenterology 131: 1400, 2006).
Sessile serrated adenomas usually bear mutated BRAF, and when dysplasia has appeared, we believe abnormal methylation has begun. The sessile serrated adenoma is considered the precursor for the "serrated pathway(s)", with mutated BRAF and high-level CpG island methylation (CIMP-H) which inactivated MLH1 and/or MGMT (paths to MSI cancers -- and is one of the routes to high-level microsatellite instability BRAF+/CIMP+/MSI cancers) or some unknonw gene (a path to BRAF+/CIMP+/MSS cancers). See Gastroent. 138: 2088, 2010.
* Less often, the lesions harbor mutated KRAS. Several genes in a senescence-related pathway have been found mutated in subjects with multiple sessile serrated adenomas (Gastroenterology 146: 520, 2014).
TRADITIONAL SERRATED ADENOMAS are actually much less common than today's usual "serrated adenomas";
The traditional serrated adenoma is more likely to harbor mutated KRAS than mutated BRAF. They may also be CIMP-H, but the cancer pathway to which they seem to belong leads to low-level microsatellite instability (MSI-L) or microsatellite-stable cancer.
* A proposed system for grading "serrated dysplasia" (Am. J. Clin. Path. 123: 349, 2005):
* Cronkhite-Canada syndrome, an obscure, non-inherited polyposis syndrome with unknown genetics (i.e. perhaps post-zygotic mutation expressing itself only when some environmental factor comes into play), seems to feature a progression of these to cancer (Digestion 69: 57, 2004.)
There is a familial syndrome with multiple serrated polyps ("sessile serrated polyposis"; "hyperplastic polyposis"). The gene has not yet been found; these people are at fairly high risk for colon cancer (Am. J. Surg. Path. 36: 1178, 2012; Gut 62: 404, 2013; Am. J. Surg. Path. 37: 434, 2013).
JUVENILE HAMARTOMATOUS POLYPS ("retention polyp") occur in infants and toddlers, usually in the rectum. They cause rectal bleeding and sometimes iron deficiency.
Grossly, these are pedunculated masses. Microscopically, you'll see colonic crypts that are mostly dilated and filled with mucus. Their loose connective tissue and constant exposure to feces means that they are almost always inflamed.
These polyps auto-amputate and get passed in the feces, which is convenient.
Patients with "juvenile polyposis syndrome" have lots of these little hamartomas and a somewhat increased cancer risk.
{15540} juvenile polyp protruding through anus
{15541} juvenile polyp, histology
PEUTZ-JEGHERS HAMARTOMATOUS POLYPS
These are large, firm polyps with a tree-like ("arborizing") central structure rich in smooth muscle.
These polyps occur multiply in the Peutz-Jegher anti-oncogene deletion syndrome, and may appear anywhere in the gut. (Physical diagnosticians: Look for distinctive freckles on the lips, palms, and genitals.) Contrary to classic teaching, Peutz-Jegher's patients are at increased risk for colorectal cancer and other cancers; the gene (STK11/LKB1 is now linked to various GI cancers Am. J. Path. 154: 1835, 1999). Why these seldom turn cancerous ("stuck at first base") is still mysterious despite the existence of a mouse model: Nature 419: 127, 2002.
{09342} Peutz-Jeghers polyp
* INFLAMMATORY POLYPS: Unfortunate, archaic term for pseudopolyps.
* BENIGN FIBROBLASTIC POLYPS are a newly-recognized but fairly common entity, usually seen in the sigmoid of middle-aged women. They are uniformly benign (Arch. Path. Lab. Med. 133: 1872, 2009). Let us worry about them.
TUBULAR AND VILLOUS ADENOMAS
These polyps are composed of benign-but-dysplastic cells arranged as crypts ("tubes") or villi. They lack the serrations, and the surface of the abnormal epithelium remains flat.
These adenomas (tubular, villous, or tubulovillous) are most common in the rectosigmoid, but may occur anywhere in the colon. About one person in three will have at least one of these during their lifetime.
* They probably begin as "aberrant crypt foci", which an endoscopist can spot with methylene blue dye, and which may harbor dysplasia. See NEJM 339: 1500, 1998.
One person in three will get at least one tubular or villous adenoma (Science 262: 1734, 1993).
The histology helps name the adenoma. They may be:
(1) tubular
(2) villous, or
(3) mixed tubulo-villous.
Lesions with more than 75% tubules are called tubular adenomas. They tend to be pedunculated and are the most common kind. Lesions with more than 75% villi are called villous adenomas. They tend to be sesssile. Villous areas are much more likely to turn malignant, and at least a third of villous adenomas harbor at least carcinoma-in-situ.
Actually, though, any of the three types of polyps may be (1) pedunculated (i.e., have a stalk, most typical of tubular adenomas, making them look like little raspberries), or (2) sessile (i.e., being slightly elevated without aclear stalk, most typical of villous adenomas.
Villous adenomas also tend to be larger, and some folks say that size is really what determines the risk of malignancy. Doesn't matter; tubular and villlous adenomas need to come out; if incompletely excised, they often recur.
Large sessile villous adenomas, in addition to being fertile breeding ground for cancer ("Reaganomas"), can bleed. They can also leak mucus, protein, potassium and water into the bowel, making a person sick.
The dysplastic cells of either type of adenoma are tall, crowded, with slight pseudo-stratification of nuclei.
{15519} normal colon vs. dysplasia in an adenoma
When the cells themselves start piling up, the nuclei show marked stratification or very big nuclei, or the cells show frequent mitotic figures, and/or form glands within glands, the pathologist will probably mention this as "high grade dysplasia" or perhaps "adenocarcinoma in situ". ("Repeat endoscopy soon" or "we hope you got it all" -- nobody knows exactly what to do). If a desmoplastic stromal response is present, we will always diagnose cancer.
Since the mucosa of the large intestine, down through the muscularis mucosae, has no lymphatics (why is this good?), colon cancer cannot metastasize until it reaches the submucosa. Until then, it's called "carcinoma in situ" or (I think better) "intramucosal carcinoma", and the pathologist will so indicate. (Anywhere else, "carcinoma in situ" means "not yet through the basement membrane").
{15547} colon polyp (a villous adenoma)
{46461} pedunculated tubular adenoma
{15499} pedunculated tubular adenoma
{09284} sessile villous adenoma (on the right)
{50560} sessile colon polyp
{15500} sessile colon polyp
{15503} tubulovillous adenoma
|
|
|
|
|
|
![]() Tubulovillous colon polyp
Tubulovillous colon polyp
Ed Uthman MD
Wikimedia Commons
FAMILIAL POLYPOSIS COLI SYNDROME
Affects one person in 8000. This includes defects in the APC locus (the common variety), in which literally thousands of tubular and villous adenomas develop in the colon early in life, and the more severe GARDNER'S SYNDROME (an unusul allete at APC; polyposis coli is accompanied by minor birth defects, epidermoid cysts of the skin, and a risk for other tumors, notably of mesenchymal origin; same locus). These are both autosomal-dominant anti-oncogene deletion syndromes.
The other common locus is MUTYH. Today, gastroenterologists distinguish "classic polyposis" (more than 100 adenomas; almost all have mutated APC) from "attenuated polyposis" (20-99 adenomas; later onset of cancer, near-equal numbers with mutant APC and mutant MUTYH -- update JAMA 308: 485, 2012). Patients with one of these syndromes have a 100% chance of eventually having one or more polyps turn malignant. Early colectomy is a good idea.
TURCOT'S SYNDROME is features with colon polyps and brain tumors. The genes may be the APC locus ("type II Turcot's"; gives mostly medulloblastomas), one of the Lynch loci (gives mostly glioblastomas NEJM 332: 839, 1995) PMS2 (Oncogene 19: 1719, 2000) or both.
* Cowden's also carries significant risk of benign and malignant colon tumors (Mayo Clin. Proc. 86: 489, 2011).
COLORECTAL CANCER is the third most common cancer and second leading cancer killer for both US men and US women, having surpassed both prostate cancer as a killer of men and breast cancer as a killer of women in the late 20th century. It is almost always an adenocarcinoma, and death from colorectal cancer is almost entirely preventable.
Genetics update: NEJM 361: 2449, 2009. The era of fecal DNA testing to screen for colorectal cancer is upon us.
|
|
|
|
|
|
|
|
|
|
This cancer often arises in one of the benign neoplastic colonic polyps cited above; only recently have we started focusing on the large minority of these tumors that arise de-novo (Cancer 75(S6): 1534, 1995). The over-riding risk factors are usually cited as (1) hereditary defects in anti-oncogenes lost in colorectal cancer, some known, some unknown (nobody questions this), and (2) years of eating the typical western diet (well maybe).
* (3) would be schistosomiasis involving the colon, where it's endemic.
Despite much pontificating, nobody really knows why diet is a risk (if it really is).
* Everything since has been in obscure journals. A "meta-analysis" finds that the main problem is the heme iron (!) and that the extra risk from being a hard-core meat eater isn't more than 20% (Meat Science 89: 310, 2011 -- "should we become vegetarians, or can we make meat safer?"). The British want us to take calcium carbonate to neutralize the heme (Br. J. Nutr. 105: 384, 2011). No link to meat, smoked or not, whatsoever in Shanghai: Nutr. Cancer 61: 194, 2009.
The old "high fat in the diet" business seems discredited -- has received almost no attetion in the 21st century, with the exception of one big Swedish study that seemed to show that eating a lot of high-fat dairy products actually seems to protects Swedes from colorectal cancer (Am. J. Clin. Nutr. 82: 894, 2005).
Even the received wisdom that low-fiber diets place you at risk (which several previous studies have failed to demonstrate) flunked a major test: NEJM 340: 169, 1999 (also NEJM 342: 1156, 2000).
The NYU team did a cross-Europe study and ended up finding no apparent link between colorectal cancer and diet (Am. J. Clin. Nutr. 80: 1003, 2004).
By 2012, almost nobody was looking at diet and colorectal cancer any more. Folate supplementation failed to prevent colorectal cancer, though one group found that folks who had relatively little folate in their diet tended to have more mutated p53 cancers (Gastroent. 135: 770, 2008), and a study on types of vegetables just added to the confusion (JADA 111: 1479, 2011 -- no striking findings, but broccoli-eaters have less right-sided colon cancer, carrot eaters have less left-sided colon cancer...)
HNPCC germline mutations ("hereditary non-polyposis colon cancer", Lynch's syndrome) confer major risk. Cloned: Nature 366: 722, 1994. They turn out to be the genes for repair of DNA mismatches ("MMR", mismatch-repair) (review the "Neoplasia" handouts if you like.) One person in 200 is born with one copy knocked out, and is at risk (upon the knocking-out of the second copy in a colonic epithelial cell) for cancers of the colon (* also ovary, uterus, and kidney and more). In the era of "personalized cancer medicine", testing for Lynch mutations in germlines and tumors has become commonplace, along with some follow-up; this is still arcane but will be important when you are in practice (Am. J. Clin Path. 137: 847, 2012).
The "MSI (microsatellite instability) status" of a tumor is turning out to be a big deal... many people without hereditary Lynch's have colorectal cancers with a mutated Lynch gene, and it's worth distinguishing these as the prognosis is supposed to be better and they are more likely to respond to 5-fluorouracil (Am. J. Path. 158: 158: 527, 2001; NEJM 249: 247, 2003 -- update Gastroenterology 146: 401, 2014). Staining for Lynch loci ("mismatch repair immunohistochemistry) when positive most often shows up absent MLH1 and PMS2. Update Adv. Anat. Path. 16: 405, 2009.
* Tipoffs that a cancer may be microsatellite-unstable include lots of infiltrating lyphocytes, right-sided location, Crohn's-like host response, mucin lakes, and absence of "dirty necrosis" (Am. J. Surg. Path. 27: 563, 2003).
* What this will mean in the long run is still unclear, but it's guiding therapy -- for example, MSI-H patients are likely to receive irinotecan (a topoisomerase inhibitor) rather than fluorouracil.
* "MYH/MUTYH-associated polyposis" results from inheriting two bad alleles at the MYH/MUTYH location, which for some reason causes G:C --> T:A transversions, notably in APC and K-ras. Patients get numerous polyps, both hyperplastic-serrated and tubular-villous-adenomatous and plenty of colorectal cancers. See Gastroenterology 135: 2014, 2008. The clinical syndrome looks like late-onset ("attenuated", 20-99 polyps) familial polyposis coli.
* Anther molecular type of colorectal cancer is "CpG island methylator" variant (CIMP+) -- sheets of cells, cribriform areas, no corkscrew glands as in most other colorectal cancers, aggressive behavior (Am. J. Surg. Path. 29: 429, 2005). We believe this arises from from the sessile serrated adenomas.
Today, we talk of "the three pathways" by which colon cancer arises.
* Future pathologists: If a Lynch pathway cancer has mutated BRAF, the patient probably does NOT have germline Lynch syndrome, but instead has had both MLH1 loci knocked out by promoter hypermethylation (Am. J. Clin. Path. 140: 177, 2013.)
Of course, prior radiation for prostate cancer much increases the risk for subsequent rectal cancer (Ann. Surg. 254: 947, 2011).
There is presently much interest in the chemoprevention of colorectal cancer. Aspirin (in the protect-your-coronaries doses) or other NSAIDS has been said to cut the rate of colorectal cancer by about 50%. This is good news, and has held up. NSAIDS are now routinely used and can cause polyps to regress, even in the familial syndrome; evidently prostaglandin E2 is the mitogen and allowed continued selection for the mutant clone (NEJM 354: 761, 2006). See NEJM 333: 609 & 636, 1995; Proc. Nat. Acad. Sci. 95: 681, 1998; NEJM 348: 883 & 891, 2003; Lancet 362: 230, 2003. COX2 inhibitors help: NEJM 342: 1946, 2000. Sulindac and an epidermal growth factor receptor kinase inhibitor: Nat. Med. 1024: 974, 2000. The cancers that are prevented are the common type that overexpresses COX-2 (NEJM 356: 2131, 2007). PIK3CA mutation that means aspirin will help prevent colon cancer: NEJM 367: 1596, 2012; BRAF-mutation means aspirin will be less helpful JAMA 309: 2563, 2013. A claim that vitamin D plus calcium would prevent colon adenomas failed a controlled study miserably: NEJM 373: 1519, 2015.
The majority (70%) of colorectal cancers, like the polyps from which many of them arise, occur in the rectosigmoid.
Tumors here typically present as narrowing of stool caliber. Of course, they begin as polypoid lesions and turn to ulcers. But by the time they're detected clinically, it's common to see the cancer growing circumferentially around the wall of the bowel ("napkin ring"; radiologists see "apple cores").
Masses in the cecum grow as huge, fungating masses. They are likely to produce iron deficiency anemia.
Eruption of multiple seborrheic keratoses is "the sign of Leser-Trelat" and warns of an occult colorectal cancer. Be alert to this.
As noted, almost all colorectal cancers are adenocarcinomas. Most are composed of tall cells making large glands, similar to those seen in adenomas ("the enteric type").
MUCINOUS CARCINOMA features lakes of mucin making up half or more of the tumor, containing clusters of cancer cells and/or signet-ring cancer cells. It tends to present at high stage and to be quite aggressive. * Again, its genetic signature tends to be different (serrated or Lynch pathway Int. J. Cancer 118: 2765, 2006).
Prognosis is most dependent on the clinical and microscopic stage, with histologic grade being of less importance. The grading system system developed by Compton (Cancer 88: 1739, 2000; Arch Path. Lab. Med. 124: 979, 2000) showed itself recently to be a significant independent prognosticator when controlling for stage (Cancer 103: 2163, 2005).
As you would expect, colorectal cancer spreads first to the regional nodes, then to the liver. Involvement of the lungs and bones is also common, and the tumor can eventually go most anywhere.
* At the same time, tomorrow's pathologist may routinely look for micrometastases using cytoketain stains (CK-IHC; Ann. Surg. 246: 568, 2007) and/or assays for mRNA of guanylyl cyclase C (! J. Clin. Path. 63: 530, 2010) or mutant k-ras (!! Ann. Surg. 251: 1087, 2010). Whether this actually has any impact on whether or not to treat is up-in-the-air right now.
* If the disease metastasizes, today's oncologists are typing KRAS, BRAF, PI3KCA, and PTEN and if all four are non-mutated, there's a good chance of response to anti-EGFR targeted therapy. There is even talk of curing colorectal cancer that's metastasized to the liver with a combination of today's targeted chemotherapy and aggressive surgery. Stay tuned.
* Future pathologists: We now have an antibody that stains specific mutated BRAF and works as well as the DNA techniques: Cancer 119: 2765, 2013.
Future pathologists: When you get a resected colon, please note all of the following (we want to know these to guide treatment; Arch. Path. Lab. Med. 132: 1600, 2008):
Future clinicians: Most colorectal cancers produce carcinoembryonic antigen. The more advanced the disease, the more likely is the CEA to be elevated. It's not suitable for screening, but draw a level on your patient with known colorectal cancer before you operate. If it comes back, the cancer is back also.
* Future pathologists: Medullary and undifferentiated enteric carcinomas can show neuroendocrine differentiation. No one knows that this means. There is also a true neuroendocrine aggressive cancer of the colon; thankfully it is rare.
* The results of chemotherapy for advanced colorectal cancer seem to be improving some. Cetuximab and panitumumab (anti-EGFR antibodies) shows promise in combination chemotherapy, if and only if the cancer does not have mutated k-ras (NEJM 360: 1408, 2009; Arch. Path. Lab. Med. 133: 1600, 2009); Gut 60: 116, 2011. Why might that be? Watch for more specific biomarkers.
KNOW: Arch. Surg. 144: 835, 2009. In 1990, adjuvant chemotherapy for stage II colorectal cancer was recommended "only for patients in studies." This is where it's remained, with some studies suggesting a slight benefit. In 2009, the surgeons and surgical oncologists looked at results of patients with stage II colorectal cancer who were offered adjuvant chemotherapy. The results speak for themselves. "The five-year disease-free survival was 50% for patients with stage II disease who underwent chemotherapy vs 76% for those who did not (P=.02). In the group negative for microsatellite instability and lymphocyte infiltration, 5-year disease-free survival was 29% for those undergoing chemotherapy and 91% for those who did not." There is probably a confounding variable or two (perhaps even a pathologist's unscientific impression that "this tumor looks aggressive, maybe you should hit it with chemo"), but the authors of the paper included the understatement of the year: "The results of the current study suggest that adjuvant chemotherapy may actually harm patients with stage II colorectal cancer."
Future pathologists: If you find metastatic cancer with an unknown primary, CK20+, CK7-, CDX2 positivity is a pretty good sign it's colorectal cancer.
{39680} adenocarcinoma of the colon ("napkin ring")
{09839} adenocarcinoma of the colon
{10540} adenocarcinoma of the colon, cross-section;
note metastases in the lymph nodes
{15456} adenocarcinoma of the colon
{19565} adenocarcinoma of the colon ("napkin ring")
{19567} adenocarcinoma of the colon, histology;
note cribriform "swiss cheese" pattern
{49225} adenocarcinoma of the transverse colon;
anus is at bottom
{20231} adenocarcinoma of the colon, histology
{23887} adenocarcinoma of the colon, stained for CEA
{39598} adenocarcinoma of the colon, perineural invasion
|
|
SECONDARY TUMORS OF THE GI TRACT
Only lung cancer and melanoma show much tendency to metastasize to the bowel mucosa. GI bleeding often kills melanoma patients.
Cancers of bladder, ovary, and cervix tend to invade the bowel directly.
AT THE END
ANAL FISSURES, or cracks in the mucosa, usually following trauma from constipation or having something inserted, are exquisitely uncomfortable.
ANAL FISTULAS may result from infection or Crohn's disease.
PERIANAL ABSCESSES occur in Crohn's disease and in people who have difficulty fighting infection (remember diabetics).
PRURITUS ANI, or intractable itching of the hindquarters ("pruritUs" means "itchy"), is a vexing problem with many different etiologies; ask a dermatologist.
ANAL CONDYLOMAS: Fairly common indicator of HPV infection.
{40364} anal condylomas
![]() Anal condyloma
Anal condyloma
Wikimedia Commons
* Those with nothing better to read may find a world-literature review of foreign bodies in the rectum in Surgery 100: 512, 1986. Zoophilia: Injury 33: 367, 2002.
There's plenty of proctocolitis due to SYPHILIS and/or LYMPHOGRANULOMA VENEREUM nowadays (Am. J. Surg. Path. 37: 38, 2013). Probably it's a good idea to stain for the spirochetes.
ANAL CANCER (review NEJM 342: 792, 2000; Arch. Path. Lab. Med. 134: 1601, 2010) is usually squamous-cell and is clearly caused by HPV infection, which is likely to be present elsewhere. It typically occurs in men or women who engage in passive, unprotected anal intercourse (Am. J. Ob. Gyn. 205: 115, 2011). The epidemiology is mostly that of a sexually transmitted disease (NEJM 337: 1350, 1997), and HPV is a major risk factor, especially type 16.
BASALOID CARCINOMA ("cloacagenic") supposedly arises from the transitional zone between anoderm and colonic-type mucosa, and looks like a basal cell carcinoma. EXTRA-MAMMARY PAGET'S DISEASE arises from adenocarcinomas of skin adnexal structures, and MELANOMAS sometime develop even where the sun doesn't shine.
* One of the most sickening tales in the annals of junk science was the "Cleveland Sex Abuse Scandal" of 1987. It began with an article in Lancet 2: 792, 1986 entitled "Buggery in Childhood". The authors documented anal findings in kids who had been penetrated anally, and reported their impression (no controls) that if the anus dilated instead of puckered, the kid had been the victim of anal sexual abuse. Dr. Marietta Higgs, a child abuse investigator, began using "reflex anal dilation" (i.e., the anus opens instead of puckers when the skin is stroked) as an indicator of child abuse. Other clinicians began "screening all children that they saw for any reason". A series of accusations, child removals, and arrests resulted. In at least a few cases, the obviously-bogus "reflex anal dilation test" was the sole basis for the accusation. "The social workers who did 'disclosure work' equated a negative history with 'denial.'" (Am. J. Dis. Child. 143: 651, 1989). This was followed by a media circus in which Dr. Higgs was variously portrayed as heroine and witch-huntress. In the aftermath, with a major court inquiry, the Lord Justice found the truth lay between the extremes. In the early 2000's, I attempted (unsuccessfully) to obtain the release from prison of a man convicted in Rhode Island of sodomizing his child, a conviction based solely (if I recall correctly) on the "reflex anal dilation test" evidence. The testimony of the American "sex abuse nurse examiner" in the early 1990's revealed she was completely ignorant that the test was discredited -- however, there was nothing I could do post-conviction. For more on this, see Arch. Dis. Child. 63: 1010, 1988 ("It has never been good medical practice to rely on just one physical sign.")
* Internet photos of toxic bowel settlement passed following "therapy" by colonic irrigation are actually blood clots. The obvious cause of the acute bleeding would probably be trauma to the bowel by the irrigation procedure. You have been warned.
 Cloacogenic carcinoma
Cloacogenic carcinoma
Pittsburgh Pathology Cases
* You thing of no bowels!"
PERITONEUM: Worth knowing
![]() Neglected peritonitis with
Neglected peritonitis with
neutrophils and necrosis
One of my autopsies
HOLLOW-ORGAN PAIN is crampy-colicky and poorly-localized; patients tend to squirm. PERITONEAL PAIN (remember it's the PARIETAL peritoneum that feels it most sharply) is knife-like and is exacerbated by movement (the patient lies still).
PERITONITIS can and does follow most intra-abdominal catastrophes. Most any bacterium can do it; fortunately, gas gangrene is rare. SPONTANEOUS BACTERIAL PERITONITIS: In cirrhotics, think E. coli or enterococcus. Nephrotic syndrome: think pneumococcus. Infection can linger as abscesses below either leaf of the diaphragm, below the liver, or in the lesser sac. Old peritonitis can organize as adhesions, just as occur after surgery. Everybody with FAMILIAL MEDITERRANEAN FEVER will have at least one bout of peritonitis.
![]() Suppurative peritonitis
Suppurative peritonitis
WebPath Photo
{39721} peritonitis, acute
{42229} peritonitis, with lots of fibrin & pus
{49191} peritonitis, after appendicitis
Prothecal peritonitis
Pittsburgh Pathology Cases
|
| 
|
PSEUDOCYST: A lesser sac or other cavity with its wall digested by lipase from a damaged pancreas.
RETROPERITONEAL FIBROSIS ("sclerosing retroperitonitis") is metaplasia of the loose connective tissue behind the peritoneum into dense, keloid-like scar. This is lethal if the ureters become pinched off. It may be idiopathic, or follow overuse of ergot for headache, or an expression of the being-sorted-out IgG4 family of diseases. SCLEROSING MESENTERITIS is another IgG4 disease.
Although most cancer in the peritoneum is metastatic, primary cancer arising here mimics serous cancer of the ovary.
MESOTHELIOMA of the peritoneum is often (but not always) an asbestos-related disease. Contrary to "Big Robbins", there's no mystery about how the asbestos reaches the peritoneal cavity; the fibers have sharp ends and can be propelled through constantly-moving tissues quite effectively.
* DESMOPLASTIC ROUND CELL TUMOR is a Ewing's variant with t11:22 / EWS/WT1.
PSEUDOMYXOMA PERITONEI: The primary is usually in the appendix, ovary, or pancreas
POST-SCRIPT
SORTING OUT FOOD POISONING: A guide for future physicians and victims (after Chandrasoma).
You ingested a bug that then made toxin
E. coli
Water, tacos from street vendors, anything else. Diarrhea in 24-72 hours.
C. perfringens
Ill-cooked food. Diarrhea in 8-14 hours.
Vibrio cholerae
Epidemic. Really bad diarrhea. This can kill anybody unless their fluids and electrolytes are managed.
Vibrio parahemolyticus
The raw oyster bug. Vomiting, diarrhea, fever in 8-96 hours.
You ingested a bug that then invaded
Salmonella
Water, poultry, shellfish, most anything else. Fever, vomiting, diarrhea in 8-24 hours.
E. coli
Enteroinvasive type. Diarrhea in 8-96 hours.
You ingested pre-formed toxin
Staph. aureus
Dairy products, custards. Impressive vomiting in 2-4 hours; works on the nerve endings in the foregut. Ever had it? Betcha you have. Beware, toxin is heat-stable.
Bacillus cereus
The fried-rice bug. (* Fried rice is made from boiled rice, which may be allowed
to stand at room temperature for a long time to avoid clumping. The fast-frying
does not kill the bug or its toxin.)
Vomiting / diarrhea in 2-14 hours. Beware, toxin is heat-stable.
C. perfringens as above.
C. botulinum![]()
Sausage, ill-canned goods. Paralysis in 24-96 hours. This can kill you.
* THE COW'S MILK FLAP
Somebody will ask you. Here goes.
On the plus side, cow's milk is (1) cheap and (2) generally pretty nutritious.
On the minus side, cow's milk is (1) kind of low in iron compared to Mom's, (2) an allergen for maybe 5% of kids under twelve months and only a few older ones, (3) still alleged by one group to be the autoantigen in type I diabetes (after a series of negative studies including JAMA 276: 609 & 647, 1996, NEJM 329: 1853, 1993, and J. Clin. Endo. 87: 3192, 2002; only the Finnish group seems still to believe this, but they're adamant: Diabetes 49: 1657, 2001), and (4) anathema to breast-feeding militants, vegans, and animal-rights activists.
That's the facts. A fad in the 1980's attributed most-if-not-all problems of young children to feeding cow's milk. The risk of the kid really being allergic to cow's milk probably still justifies pediatricians recommending withholding cow's milk from all babies until the first birthday. However, the claims of harm went much farther. The science obviously took back seat to the politics. Most of the shouting-and-pouting has died down, studies examining various supposed risks of cow's milk keep coming up negative (introducing cow's milk earlier doesn't really cause allergies later: Arch. Dis. Child. 86: 365, 2002; doesn't cause obesity later JAMA 285: 2461, 2001).
Some kids are allergic to cow's milk, which gives them diarrhea and belly cramps and even hemorrhage ("cow's milk protein-sensitive enteropathy"; J. Ped. 139: 797, 2001 based on morphology and recognizing widespread skepticism exists; Arch. Dis. Child. 68: 240, 1993). There are a host of lab tests offered for diagnosis; the best test is probably to withhold milk for a while, then give a challenge dose. Patch testing is so-so: J. Ped. 142: 203, 2003.The mechanism seems to be type IV immune injury, with sensitized round cells producing interferon, alpha-TNF, and so forth (Gastroenterology 106: 1514, 1994). Normal kids' round cells do the same thing but only about half as much, if we believe this study. Some folks even claim that if Mom drinks cow's milk, its antigen is transferred to her blood and milk and this makes her baby sick (this is a little hard to believe, but the transfer does seem to happen: J. Allerg. Clin. Imm. 93: 787, 1994; Gut 34: 203, 1993; Arch. Dis. Child. 66: 300, 1991; Pediatrics 87: 439, 1991). A single instance in Poland of a child with apparent life-threatening events (i.e., stops breathing; some people think this is related to SIDS and some do not) and one anomalously high level of casomorphin in the blood (it is inexplicably, tremendously elevated unlike any other child's -- lab error? metabolic kink?) stops having the events after Mom stops drinking cow's milk (J. Ped. Gast. Nutr. 52: 772, 2011) is now being touted as proof that cow's milk consumption by Mom causes SIDS. However, opiates and opiate-peptides cause slowing of respiration, not sudden stoppage. Watch this one.
RAST demonstrating allergy to cow's milk predicts that a kid's atopic eczema will benefit from eliminating cow's milk (same for eggs: J. Allerg. Clin. Imm. 91: 658 & 668, 1993). A prospective study found that where the allergen isn't obvious, kids' IgE-mediated symptomatology isn't reduced by eliminating cow's milk either late (Arch. Dis. Child. 68: 724, 1993) or from the beginning of life (Arch. Dis. Child. 67: 1008, 1992), or before birth (J. Allerg. 89: 709, 1992). A huge review finds that dairy doesn't raise inflammatory biomarkers in overweight / obese adults (Am. J. Clin. Nutr. 97: 706, 2013).
See also Arch. Ped. 146: 1432, 1992; 148: 104, 1994, by an author who recognizes the faddism and the reality. New Zealand (where "progressive ideas" tend to be very popular) now has enough young adults who were denied milk through their childhoods and did not calcium-supplement are having many, many more fractures and are much fatter than their peers (JADA 104: 250, 2004.) And of course, thanks to the fad, rickets is back in oh-so-modern England (Lancet 362: 1389, 2003). Diagnosing a kid with allergies (whether or not the kid actually has allergies) puts the kid at serious risk for stunted growth unless you follow up meticulously (JADA 102: 1648, 2002). Feeding cow's milk to newborns: Pediatrics 91: 515, 1993. Mostly about iron, from the pediatric think-tank: Pediatrics 89: 1105, 1992. Rifkin's "environmental activists" held up for over a decade (disinformation campaigns, boycott threats, smear tactics) the widespread use of bovine-somatotropin to enhance production of cow's milk, which increases yields by around 20%; it was declared safe by the FDA in 1985 (JAMA 264: 1003, 1990) but thanks to activism remained unused for many more years. Concerns about the treatment promoting bovine mastitis floundered with studies (J. Dairy Sci. 82: 1465, 1999, J. Dairy Sci. 82: 1671, 1999) actually diminishes the frequency and severity of the infections. But the disinformation campaign by animal-rights people, militant vegetarians, and anti-biotechnology activists continues. I would be willing to pay substantially more money to know that the animals I eat were raised and treated humanely. I suspect the reason that this has (sadly) not happened is that the public perceives that concern for feed animals to belong to the lunatic fringe that dominates animal-welfare activism ("Exploitation!" "Murderers!" "Species discrimination!" "Far worse than the Holocaust!"). Let me know if you have any insight into this puzzling phenomenon, and if you have a chance to choose to pay more for a free-range chicken, do it. And think... just how many sweet and gentle cows would there be if there weren't a market for beef, dairy products, and leather? What would the world be like without carnivores? No life forms higher than bacteria. And do you really want America's grazing land littered with the rotting bodies of cattle and buffalo herds while much of the rest of the world is hungry? That's reality, people. As a physician, it seems to me that you have a duty to help people sort out and see through the beautiful bad ideas that are likely to hurt them and hurt society. Don't ignore it. Be responsible.
* Serious evidence for the effectiveness of acupuncture in
GI disease is conspicuous by its absence. Even the Chinese
now admit that it's best reserved for patients that you can't help
by any established method (Gut 51: 617, 2002).
PETA's merchandising campaign "Got pus? Milk does" reflects the fact that dairy cattle may have bacterial infections of the udders, just as a nursing mother may. Of course, milk is one of the most regulated products, and must be pasteurized. It is ironic that the scientifically-illiterate targets of this campaign are the same people who are targeted by anti-pasteurization disinformation.
In 2008, the World Health Organization published Safer Water, Better Health. It is a good read, and is intended to persuade those in power to make the drinking water supply safe in the poor nations. This time, the WHO wisely appealed to the greed of the governments and entrepreneurs of the poor nations, calculating a payback of $84 billion in better employee performance etc. for the $11 billion annual investment for water treatment. See Lancet 371: 2145, 2008.
*
SLICE OF LIFE REVIEW

{08789} small bowel, normal
{08790} small intestine normal
{10163} duodenum, normal
{10502} colon, normal mucosa
{11740} stomach, normal
{11741} colon, normal
{11742} colon, normal
{11744} appendix, normal
{11745} appendix, normal
{11804} bowel, normal
{11808} bowel, normal
{11810} ileocecal valve and bowel, normal
{14829} esophagus (esophageal gland), normal
{14830} esophagus (esophageal gland), normal
{14831} esophagus (esophageal gland), normal
{14832} esophagus (esophageal gland), normal
{14833} stomach body, normal
{14834} stomach body, normal
{14836} stomach body (gastric glands), normal
{14837} stomach body (pits & glands), normal

{14838} stomach body (pits & glands), normal
{14839} stomach body (glands), normal
{14840} stomach body (glands), normal
{14841} stomach pylorus (pits & glands), normal
{14842} stomach pylorus (pits & glands), normal
{14843} duodenum (brunner's glands), normal
{14845} duodenum (brunner's glands), normal
{14847} brush border, intestine
{14848} brush border, intestine
{14849} villus, normal intestine
{14850} villus, normal intestine
{14851} crypt of Lieberkuhn, normal
{14852} crypt of Leiberkuhn, normal
{14854} enterochromaffin cells, normal
{14855} villi, jejunum
{14857} Auerbach's plexus
{14859} Meissner's plexus
{14862} Peyer's patches ileum
{14863} appendix, normal
{14865} colon, normal
{14868} colon (crypt), normal
{14869} colon (crypt), normal
{14870} anal rectal junction, normal
{14871} pectinate line, anorectral junction
{15090} ileum, Peyer's patches
{15094} ileum, Peyer's patches
{15095} ileum
{15096} rectum
{15097} rectum
{15100} jejunum, normal
{15101} jejunum, normal
{15102} rectum
{15103} rectum
{15175} esophagus
{15176} esophagus
{15177} esophagus
{15178} esophagus
{15179} esophagus
{15182} stomach, body
{15183} stomach, body and pylorus
{15184} stomach, body and pylorus
{15185} stomach, body and pylorus
{15186} stomach, body and pylorus
{15204} duodenum
{15206} duodenum
{15207} duodenum
{15208} duodenum
{15236} appendix
{15238} esophagus, gland
{15239} esophagus, duct and gland
{15242} esophagus, lymphocyte aggregate
{15243} stomach, cardia
{15244} stomach, cardia
{15245} stomach, cardia
{15246} stomach, body
{15247} stomach, body
{15248} muscularis mucosa, stomach
{15249} auerbach's plexus, stomach
{15250} meissner's plexus, stomach
{15251} lamina propria, stomach
{15253} surface mucus cells, stomach
{15254} stomach, venule
{15255} stomach, pyloric/body junction
{15256} stomach, pyloric/body junction
{15257} jejunum, normal
{15258} jejunum, crypts
{15259} jejunum, terminal bars (tb)
{15260} paneth cell, jejunum
{15261} brunner's gland, duodenum
{15262} brunner's gland, duodenum
{15264} auerbach's plexus, duodenum
{15266} appendix, lymphocyte aggregate
{15267} peyer's patch, ileum
{15268} peyer's patch, ileum
{15269} lamina propria, ileum
{15270} colon, normal
{15271} colon, normal
{15272} colon, lymphocytes
{15273} colon, taenia coli
{15329} ileum, Peyer's patches
{15581} stomach, normal unfixed
{15582} stomach, rugae unfixed
{15584} stomach, normal unfixed
{15586} stomach, normal
{15595} small bowel unfixed, normal
{15596} small bowel unfixed, normal
{15597} small bowel unfixed, normal
{15598} small bowel unfixed, normal
{14835} stomach cardia, normal
{16505} tonsil, normal
{17557} appendix, normal
{19365} jejunum, normal
{19366} jejunum, normal
{19368} jejunum, normal scanning EM
{19450} esophageal gastric junction, normal
{19494} jejunum, normal
{20842} stomach, cardia
{20868} valve of kerckring, duodenum
{20878} taenia coli, colon
{24412} duodenum, normal
{24413} small intestine, normal
{24423} appendix, normal
{24424} appendicitis and normal appendix
{24432} polyp, adenomatous and normal colon
{24810} appendix, normal
{24811} appendix, normal
{25463} esophagus, normal
{49192} appendix, normal
BIBLIOGRAPHY / FURTHER READING
I urge anyone interested in learning more about diseases of the GI tract to consult these standard textbooks.
In my notes, the most helpful current journal references are embedded in the text. Students using these during lecture strongly prefer this. And because the site is constantly being updated, numbered endnotes would be unmanageable. What's available online, and for whom, is always changing. Most public libraries will be happy to help you get an article that you need. Good luck on your own searches, and again, if there is any way in which I can help you, please contact me at scalpel_blade@yahoo.com. No texting or chat messages, please. Ordinary e-mails are welcome. Health and friendship!

| New visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if people like me who call ourselves Christians didn't try to act as good as other good people ." Prayer Request

| If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |
Teaching Pathology
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |
 |
Click here to
see the author prove you can have fun skydiving without being world-class. Click here to see the author's friend, Dr. Ken Savage, do it right. |


