Clinical Scenario: 62 y.o. African American male presents with RUQ abdominal pain with 18 lbs of weight loss over a two month period and pruritus. The patient describes the pain as “a dull ache that radiates straight through to his back.” The pain comes and goes and is worse upon eating. The patient also appears jaundiced. He denies any N/V/D/C but says that his stool is “light, on the tan side, and smells terrible.” The patient describes his diet as “meat and potatoes when he feels like eating.” He has smoked since he was 20 y.o. about 1 ppd. He admits to drinking daily at least a 6 pack. Past medical history includes chronic pancreatitis and uncontrolled diabetes mellitus of less than a year. Family history of cancer is negative. There are NKDA. Physical exam shows a cachexic man 6’0" and weighing 115 lbs. There is odor of ethanol on the patient’s breath. Temperature is 99.0 F, pulse 90, respirations 18 and BP 145/100.
Labs: Ultrasonography, Computerized Tomography, Magnetic Resonance Imaging, Magnetic Resonance Imaging with guided percutaneous fine-needle biopsy, Endoscopic Retrograde Cholangiography (ERCP), Endoscopic Ultrasonography (EUS), tumor marker determination (CA 19-9, DU-Pan 2, CEA, Span-1), and Fine Needle Aspiration (FNA).
Lab Results: Pancreatic ductal adenocarcinomas on US are echo-poor and inhomogenous mass lesions (80%). With increasing size, tumors become inhomogenous with cystic and echo-rich areas. EUS lymph node metastases appear as enlarged echo-poor nodes. ERPC demonstrates displacement, narrowing, or obstruction of the pancreatic duct. CT shows hypodense masses.
Gross: Firm and poorly defined masses. Cut surfaces are yellow to white. Hemorrhage and necrosis uncommon, but microcystic areas may be found. Carcinomas of the head of the pancreas usually invade the common bile duct and/or main pancreatic duct and produce stenosis that results in proximal dilation of both duct systems. Complete obstruction of the main pancreatic duct leads to extreme prestenotic duct dilation with duct haustration and fibrous atrophy of the parenchyma. More advanced pancreatic head carcinomas involve the ampulla of Vater and or duodenal wall, causing ulcerations. Tumors of the body or tail obstruct the main pancreatic duct, but typically do not involve the common bile duct.
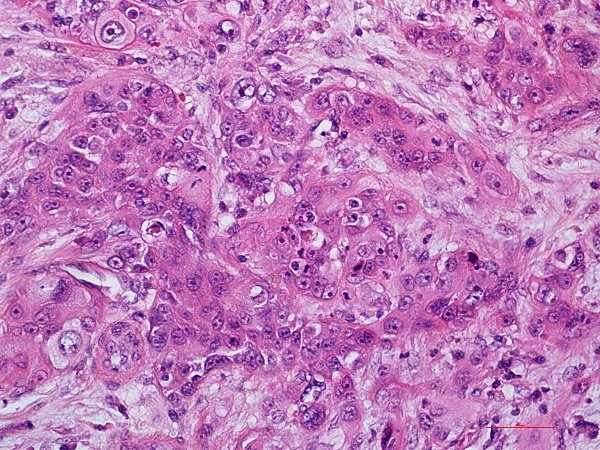
Histopathology: Poorly differentiated adenocarcinoma of the pancreas with focal squamous cell differentiation are composed of a mixture of densely packed, small irregular glands as well as solid tumor cell sheets and nests, which entirely replace the acinar tissue. While typical large, duct-like structures and intraductal tumor components are absent there is presence of variable proportions of mucin-producing glandular elements and squamous components of at least 30% of the tumor tissue. In addition there may be anaplastic spindle cell foci and scattered inflammatory cells.
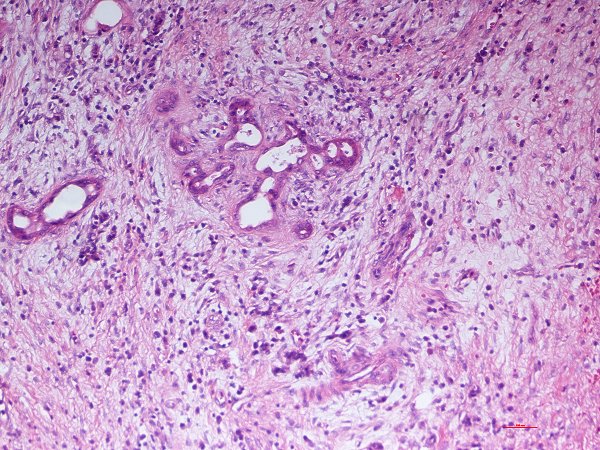
Final Diagnosis: Poorly Differentiated Adenocarcinoma of the Pancreas with Focal Squamous Cell Differentiation
Summary: Poorly Differentiated Adenocarcinoma of the Pancreas with Focal Squamous Cell Differentiation is a rare variant of pancreatic exocrine carcinoma and is a very aggressive cancer. Squamous metaplasia of the pancreatic ductal epithelium occurs most commonly in the setting of chronic pancreatitis, but is noted in the adjacent ducts of only about 4% of adenocarcinomas. Pancreatic cancer is the 5th leading cause of cancer death in the Western counties, second to colon cancer among malignancies of the digestive tract. 60-70% of pancreatic cancers are found in the head of the gland and the rest in the body and tail.
Differential: Undifferentiated (anaplastic) carcinoma of the pancreas, Undifferentiated carcinoma with osteoclast-like giant cells of the pancreas, Mucinous noncystic carcinoma of the pancreas, and Signet-ring cell carcinoma.

Georgia Leake KCUMB '15