Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com
No texting or chat messages, please. Ordinary e-mails are welcome.
|
|
 |
 |
 |
 |
|
verify here. |
Cyberfriends: The help you're looking for is probably here.
This website collects no information. If you e-mail me, neither your e-mail address nor any other information will ever be passed on to any third party, unless required by law.
This page was last modified January 1, 2016.
I have no sponsors and do not host paid advertisements. All external links are provided freely to sites that I believe my visitors will find helpful.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected. No texting or chat messages, please. Ordinary e-mails are welcome.
 I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
 If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |

|
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
 My team:
My team:
pathology.org -- my cyberfriends, great for current news and browsing for the general public
EnjoyPath -- a great resource for everyone, from beginning medical students to pathologists with years of experience
Medmark Pathology -- massive listing of pathology sites
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures
Freely have you received, freely give. -- Matthew 10:8. My site receives an enormous amount of traffic, and I'm still handling dozens of requests for information weekly, all as a public service.
Pathology's modern founder, Rudolf Virchow M.D., left a legacy of realism and social conscience for the discipline. I am a mainstream Christian, a man of science, and a proponent of common sense and common kindness. I am an outspoken enemy of all the make-believe and bunk that interfere with peoples' health, reasonable freedom, and happiness. I talk and write straight, and without apology.
Throughout these notes, I am speaking only for myself, and not for any employer, organization, or associate.
Special thanks to my friend and colleague, Charles Wheeler M.D., pathologist and former Kansas City mayor. Thanks also to the real Patch Adams M.D., who wrote me encouragement when we were both beginning our unusual medical careers.
If you're a private individual who's enjoyed this site, and want to say, "Thank you, Ed!", then what I'd like best is a contribution to the Episcopalian home for abandoned, neglected, and abused kids in Nevada:
My home page
More of my notes
My medical students
Especially if you're looking for information on a disease with a name that you know, here are a couple of great places for you to go right now and use Medline, which will allow you to find every relevant current scientific publication. You owe it to yourself to learn to use this invaluable internet resource. Not only will you find some information immediately, but you'll have references to journal articles that you can obtain by interlibrary loan, plus the names of the world's foremost experts and their institutions.
Alternative (complementary) medicine has made real progress since my generally-unfavorable 1983 review. If you are interested in complementary medicine, then I would urge you to visit my new Alternative Medicine page. If you are looking for something on complementary medicine, please go first to the American Association of Naturopathic Physicians. And for your enjoyment... here are some of my old pathology exams for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I do not accept donations, though I appreciate those who have offered to help.
During the eighteen years my site has been online, it's proved to be one of the most popular of all internet sites for undergraduate physician and allied-health education. It is so well-known that I'm not worried about borrowers. I never refuse requests from colleagues for permission to adapt or duplicate it for their own courses... and many do. So, fellow-teachers, help yourselves. Don't sell it for a profit, don't use it for a bad purpose, and at some time in your course, mention me as author and William Carey as my institution. Drop me a note about your successes. And special thanks to everyone who's helped and encouraged me, and especially the people at William Carey for making it still possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it, here or elsewhere. Health and friendship!

![]()
![]()
LEARNING OBJECTIVES:
Cervix:
Endometrium / Myometrium:
Give a full account of the etiology, pathogenesis, and clinical correlates of each of the following, and recognize grossly and/or microscopically as appropriate:
Oviduct:
Ovary:
List each of the three categories of primary ovarian tumors, and for each of these, the principal tumors and their distinguishing anatomic and clinical features, risk factors, paraneoplastic syndromes, biological behavior, and patterns of spread if applicable.
Mother and Child:
Describe how examining the placenta can sometimes help determine
whether twins are identical or fraternal.
![]() KCUMB Students
KCUMB Students
"Big Robbins" -- Female
Lectures follow Textbook
QUIZBANK
Cervix: Women's problems 80-93 Endometrium / Myometrium: Women's problems 1-12, 18, 37-59, 64-66, 69-71, 73-75, 77-79, 94-101 Oviduct: Women's problems 24-25, Ovary: Women's problems 76, 102-128 Mother and Child: Fetus and pregnancy (all) |
 Picasso, "Mother and Child" |
If I were asked to what the singular prosperity and growing strength of [the Americans] ought mainly to be attributed, I should reply, "To the superiority of their women".
-- Alexis de Tocqueville 1789
Never try to impress a woman because if you do, you'll have to keep up that standard for the rest of your life.
-- W.C. Fields
Not from Adam's brain, to have the same mind as him, nor from Adam's foot, to be subordinate to him, but from the rib next to Adam's heart, to love and be loved by him.
-- Anonymous
Let men tremble to win the hand of a woman, unless they win also with it the utmost passion of her heart.
-- Nathaniel Hawthorne, "The Scarlet Letter"
If that this thing we call the world
By chance on atoms was begot
Which though in ceaseless motion twirled
Yet weary not
How doth it prove
Thou art so fair and I in love.
-- John Hall, 1646
Global views on women's health: Sci. Am. 271(2): Aug., 1994. Still good reading, especially for anyone offering easy, wrong answers to the world's problems.
In sub-Saharan Africa, one woman in 16 dies in childbirth, compared with one woman in about 5000 in the developed world (Br. Med. J. 326: 567, 2003). British aid workers among the poor were able to cut mortality in pregnancy and delivery by about 40% with very little effort or expense (BMJ 336: 145, 2008).
The best hope for women in the resource-poor environment today seems to be other women mobilized to make their lives -- including health-care outcomes -- better. See Lancet 381: 1721 & 1731, 2013.
Special thanks to Dr. Tony Racela for the wonderful kodachromes. You may find them here.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
{47710} human female
{15787} normal internal female genitalia
|
|
Primordial germ cells from the yolk sac migrate to the ovarian (or testicular) stroma. (Some of these supposedly go astray and end up in other midline structures, explaining why "germ cell tumors" arise in the retroperitoneum, pineal, and anterior mediastinum.)
In female embryos, the mullerian (paramesonephric) ducts result from infolding of the coelomic lining epithelium. They give rise to the surface epithelium of the ovaries, and the lining of the oviducts and uterus. In male embryos, Mullerian inhibitory substance from the testis makes the mullerian ducts regress.
In female embryos, the wolffian (mesonephric) ducts regress, persisting only as little bits of epithelium along the whole female tract. These give rise to "Gardner's duct cysts" along the cervix and vagina. In male embryos, the wolffian (mesonephric) ducts become the epididymis and vas.
Only the upper two thirds of the endometrium ("the functionalis") cycles. The basal third ("the basalis") does not respond to a woman's steroid hormones and stays in place, giving rise to next month's endometrium. The theca cells surrounding the follicle are ovarian stroma that nurture a particular follicle. You can tell when they have luteinized (i.e., become hormonally active) because they plump-up and become pale-staining (from the lipid used to make steroids). There are a few Leydig-like cells in the hilus, able to make testosterone.
During reproductive life, every month several (not just one) follicles mature as graafian follicles. One ovulates and suppresses the others, and becomes a corpus luteum, which will regress when the pregnancy ends or does not occur. It will be recognizable for a few months, gradually being replaced by scar tissue.
The oviduct's mucosa has ciliated cells, secretory cells, and almost-no-cytoplasm "peg cells" ("intercalated cells"). The oviduct's mucosa is thrown up into complicated folds ("plica", or "fimbria" at the end). I've been told that the reason women have orgasms is to make the oviducts wiggle around and be sure to catch the egg if it's just been released -- and especially if it's Mr. Right. Decide about that for yourself.
On rotations youlll need to know the acronym TORCH for multifocal, chronic inflammation of the plancenta. (T is for toxoplasmosis O is for the others, notably varicella, Epstein-Barr, Chagas disease, and syphilis. R is for rubella. C is for cytomegalovirus. H is herpes simplex. In the United States, you will probably only run into CMV and syphilis.) Here is a review of the major infections of the female genital system, adapted from "Big Robbins".
HERPES SIMPLEX II![]()
You already know that herpes simplex 2 sheds from time to time even without blisters being present. Be careful (JAMA 305: 1441, 2011).
In late pregnancy or shortly after birth, inflammation and necrosis of the umbilical cord ("necrotizing funisitis") and severe damage to the newborn.
|
|
You are already familiar with the classic "herpes cell" seen on Tzanck preparation
or pap smears. Cells with multiple gigantic nuclei, usually bearing a
central viral inclusion![]() , are diagnostic.
, are diagnostic.
If herpes is transmitted to the child during birth, severe sickness, brain damage, and even death are likely to occur.
HUMAN PAPILLOMA VIRUS (HPV)
Today, screening women and men for chlamydia by nucleic acid amplification techniques is becoming a standard part of routine health care maintenance; it can be done on urine. It is fairly expensive but the payoff (preventing pelvic inflammatory disease and ectopic pregnancy) is supposed to make it cost-effective. The Swedes seem to believe it's been a major health blessing; others are not so sure (BMJ 334: 725, 2007).
{11562} chlamydia, pap smear
{25911} chlamydia infection, pap smear
|
|
* A new nucleic acid check that screens liquid pap tests for chlamydia and gonorrhea: South. Med. J. 106: 506, 2013.
HEMOPHILUS DUCREYI
MYCOBACTERIUM TUBERCULOSIS![]()
GARDNERELLA
You can make the diagnosis by observing that the vaginal pH is more alkaline than the usual 4.5.
Or you can confirm the diagnosis by adding a drop of dilute potassium hydroxide. This will accentuate the fish smell. This indicates "bacterial vaginosis", the most common cause of vaginitis and cervicitis during the reproductive years. The flora is mixed; Gardnerella is the marker species.
Gardnerella bacteria cling to epithelial cells, creating the fuzzy-looking "clue cell" in pap smear.
Gardnerella is today's "usual suspect" for producing many cases of premature rupture of the membranes, premature labor, and premature birth (Hosp. Med. 61: 475, 2000). Screening for gardnerella during pregnancy cuts prematurity dramatically: Br. Med. J. 329: 371, 2004.
* Don't confuse Gardnerella with "Bacillus vaginalis / lactobacilli / Doderlein bacilli", which live off glycogen and lyse glycogen-rich cells. Whether they are ever a problem is doubtful. A true Gardnerella clue cell looks fuzzy; lactobacilli are thick, distinct rods.
CANDIDA![]() :
:
This produces a red, itchy rash that may have fungal colonies visible. You can scrape them off and see them under the microscope. Biopsy is unnecessary. The inflammation is superficial and the infection is annoying but not (by itself) dangerous.
Contrary to "Big Robbins", I am not aware of any reason to believe that some women are more vulnerable because they are "chronic carriers". The bug is ubiquitous. Yeast infections are more likely when there is more glucose in the area (pregnancy, on the oral contraceptive pill, diabetes), or when the normal bacteria are suppressed with antibiotics.
Occasionally a candida infection of the fetus and membranes follows a tear. The most dread complication is nerosis of the umbilical cord.
TRICHOMONAS: Vulva, vagina, cervix: Trichomonas vulvovaginitis
This produces a bad-smelling, red ("strawberry") inflammation with a thin discharge. If you are inexperienced and happen to biopsy it, you'll see only superficial inflammation.
The protozoan is easily seen in wet mounts, looking like a bouncing pear moving about with wiggly flagella.
Ask a pathologist to show you a pap smear slide with "Trich"; there is often a second micro-organism, a very long filamentous bacterium called "leptothrix".
Trichomonas is much less common nowadays thanks to its incidental discovery on pap smears. As long as both partners are treated, expect a good result (Lancet 363: 545, 2004).
|
|
|
|
![]() Vulva
Vulva
"Pathology Outlines"
Nat Pernick MD
NON-NEOPLASTIC DISORDERS
LABIAL ADHESIONS are not a pathologist's disease. They are rare at birth but common in childhood, and must be the sequelae of mild inflammation. You can usually lyse them with warm water and gentle probing.
Gonorrhea and trichomonas can be acquired during birth. A little girl's NONSPECIFIC VULVOVAGINITIS may look terrible, but is likely to be the result of poor hygiene or pinworms. You'll still culture for gonorrhea and chlamydia and check for trichomonas.
VULVAR VESTIBULITIS (various names) is a pain syndrome in which the vulva becomes tender and intercourse is painful.
Ectopic breast tissue is fairly common on the vulva. It can enlarge during pregnancy and lactation.
"Acute vulvitis" is nonspecific inflammation of the vulva, by various surface bacteria.
Distinguishing vulvar cysts:
SKENE'S GLANDS, on either side of the urethra, can also become inflamed, especially by gonorrhea.
* VESTIBULAR ADENITIS is a poorly-understood inflammatory process at the entry to the vagina. The glands are inflamed and very painful. They may be excised surgically for a cure.
SKIN DISEASES including lichen simplex (simple hyperplasia of the epidermis), psoriasis, lichen planus, vitiligo, and familial pemphigoid, are very familiar on the vulva.
Sometimes the epidermis simply undergoes hyperplasia, usually without anaplasia. It thickens ("acanthosis"), and develops extra keratin ("hyperkeratosis"). We call this VULVAR HYPERPLASIA. (This is a cancer risk if an only if there is some anaplasia.) It is not clear to me where this begins and lichen simplex chronicus leaves off.
LICHEN SCLEROSUS ("chronic atrophic vulvitis"), the most common lesion on the vulva, is a mysterious process in which a band of loose, pale-staning, homogeneousouse collagen forms underneath the epidermis, which is thinned and maybe has a hydropic basal layer. The skin turns gray and parchment-like or cigaret-paper-like and becomes itchy. It can occur at any age -- even children. Although there is no anaplasia, a few percent turn malignant.
* Of course, lichen sclerosus in a child has gotten parents hauled into court, where misguided zealots say that it is "proof of child abuse": Br. Med. J. 320: 331, 2000.
Lichen sclerosus review: Lancet 353: 1777, 1999. Topical glucocorticoids seem to work better than topical sex steroids. Today, lasers are being used with good results (Derm. Surg. 30: 1148, 2004).
BENIGN TUMORS
MUCOSAL POLYPS are skin tags, fibrous nodules covered with normal epithelium.
* "Lactating adenoma" is ectopic breast tissue during pregnancy (Ob. Gyn. 118: 478, 2011); ectopic breast tissue in the vulva should be excised because of the cancer risk.
CONDYLOMA ACUMINATUM is the large, usually multiple warts that can occur on the vulva, perianal region, and (less often) the vagina and cervix.
|
|
|
|
|
Remember HPV strains 6 and 11 as causes of condyloma acuminatum (and its giant variant, "verrucous carcinoma"). Remember HPV 16 and 18 (also 31, 33, and 35) as causes of ordinary, deadly carcinoma; if strains 16 or 18 produces a wart, it is likely to be flat rather than tree-like. A woman may have several strains.
* "Who has what strain?" In preparation for tomorrow's studies of the efficacy of the vaccine, the Saskatchewan pathologists find that HPV-16's still the commonest, that there's a LOT of HPV-31 and not much HPV-18. Stay tuned (Arch. Path. Lab. Med. 132: 54, 2008).
Nowadays, you may send ladies to culposcopy if they have HPV-16 or HPV-18 even with a normal pap smear (Am. J. Clin. Path. 136: 578, 2011).
* A therapeutic vaccine TG4001 that carries HPV-16's E6 and E7 oncoproteins seems to clear dysplasia caused by HPV-16 if it's the only virus on board (Am. J. Ob. Gyn. 204: 169, 2011). Stay tuned.
* Update on HPV and cervical cancer: Lancet 382: 889, 2013.
* Leave the diagnosis of such entities as "aggressive angiomyxoma", "angiomyofibroblastoma", and "angiofibroma" to us. These are nasty-looking benign lesions, often quite large, that are prone to recur.
CARCINOMA OF THE VULVA
{25666} melanoma of vulva, gross
Most squamous carcinomas are caused by HPV, and are preceded by dysplasia and carcinoma in situ ("vulvar intraepithelial neoplasia" / "VIN"; "vulvar intraepithelial lesion" is better), which is analogous to the lesions in the cervix. A physician may notice the premalignant lesions and excise them before cancer develops.
Future pathologists: Around 40% of vulvar intraepithelial lesions are HPV-related and look like the lesions in the cervix. These tend to be multifocal. The reamining 60% are seen in older women, are usually unifocal and/or run with lichen sclerosus, and tend to light with with p53.
* Pathologists distinguish a host of subtypes of vulvar squamous carcinomas, including keratinizing (most common -- a lot of dense keratin here can be your tipoff), basaloid, spindle cell, warty, and verrucous. Don't worry about these for now.
EXTRAMAMMARY PAGET'S DISEASE is mucin-rich cancer cells growing within the epidermis of the vulva or perineum.
Local excision should be curative. The pathologist will do frozen sections to help see if the margins are free. Even without excision, the lesion is likely to remain stable for a long time.
* While surgery is still the preferred treatment, a majority of women who are not operative candidates get good results with topical imiquimod, the immune modulator (Arch. Derm. 147: 704, 2011).
* CHILD SEXUAL ABUSE
A lot of abuse,
sexual and non-sexual, goes on, and
you need to be alert. And please
remember the importance of knowing your stuff, and the dangers of a wrong diagnosis
either way. Especially, be alert
for fads -- if something doesn't make sense (i.e., the Marietta Higgs claims),
don't believe it. Even Am. J. Clin. Path. 123: S119, 2005
showcased how rampant the false-positive diagnosis of child abuse has become,
and how devastating the impact is.
You already know that (1) good medicine involves differential diagnosis
and objectivity;
(2) health care professionals are not inerrant, (3) patients
are not always "good historians", and (4) stories that change in big ways
over time are usually lies. From Salem's witchcraft
to McMartin and after, it's clear you can
eventually get a kid to say anything in court. My job would be much easier if
everybody knew all this.
As "the pathology guy", I've had several courtesy cases involving
allegations of child sexual abuse. In the majority, I've told the
attorney to have a heart-to-heart with the guilty defendant. I have
seen fine work by physicians and sex-abuse nurse examiners (SANE).
However, I've also had cases that show medical ignorance/arrogance and politics at their worst.
Adults who recall sexual abuse as children have more
psychopathology than those who do not; there's one classic
study in which when you control for their families being dysfunctional and doing many other
things that guarantee the child will have difficulty later,
the effect of the sexual stuff itself largely but not totally disappears
(J. Consult. Clin. Psych. 61: 284, 1993 -- the study was massively condemned
for political incorrectness but never discredited as far as I can tell). It would be very
hard to do a controlled study of adults who were molested by a non-family-member
vs. those who weren't; the closest is Br. J. Psych. 179: 444, 2001,
in which of course it was much worse if the abuser was a family member,
force was used, and/or intercourse occurred, and there is no specific
"post-sexual abuse syndrome" (contrast with the more narrow
spectrum of problems seen in returning combat veterans).
You'll learn on rotations how to detect child sexual abuse. The
best work was done in the 1990's after the McMartin preschool ritual abuse
fiasco -- much of it
(to her great credit) by the physician
whose overcall led to this absurd trial.
The culture of irresponsibility and self-deception in child-protection circles is starting
to gain attention from the media (KC Star March 17, 2013).
What is most disturbing about these cases is that it's essentially
impossible to find a clinician willing to testify on behalf of an
obviously falsely-accused child abuser -- it would be bad for business.
It seems to me that this is an area
where pathologists can help.
![]() Normal vagina with cervix
Normal vagina with cervix
WebPath
![]() Vagina
Vagina
"Pathology Outlines"
Nat Pernick MD
NON-NEOPLASTIC LESIONS
You are familiar with the various vaginitis syndromes. The clinical diagnosis of candida, trichomonas, and gardnerella is usually easy enough clinically. Nowadays, molecular diagnosis (DNA, colorimetric, develops in 45 minutes) is replacing pap smear for comfirmation (Am. J. Clin. Path. 135: 442, 2011).
Girls exposed in utero to diethylstilbestrol (DES) often have glands in the upper vagina. These appear as red bumps against the normally-pink mucosa. They may look like endocervical glands with squamous metaplasia, or like endometrial glands / oviduct without stroma. These turn cancerous in fewer only about 1 of 700 of affected girls ("clear-cell / hobnail" adenocarcinoma -- teenaged years, usually curable but present a major problem with reconstruction.) The long-term follow-up shows little or no additional anatomic pathology in thie cohort (NEJM 364: 2083, 2011); however there are reports of increased infertility, cervical cancer, ectopic pregnancy, miscarriage, pre-eclampsia, stillbirth, early menopause, and breast cancer (NEJM 365: 1304, 2011). Given the emotional nature of the subject, it's hard to do good work. You decide.
Maybe one girl in 5000 has aplasia/hypoplasia of the mullerian (maramesonephric) ducts (small or absent uterus and proximal vagina / "Rokitansky syndrome"). If the mullerian ducts fail to fuse, the vagina may be septate; if the urogenital sinus doesn't form properly the vagina may be atretic, and so forth.
The only common non-infectious, non-neoplastic, acquired lesion of the vagina is a Gartner duct cyst, from the Wolffian duct remnants.
|
|
|
|
CANCER OF THE VAGINA
VAGINAL INTRAAEPITHELIAL NEOPLASIA, which is of course HPV related, is now treated by surgery, lasers, imiquimod or 5-fluouracil with an excellent prognosis (Ob. Gyn. 122: 1223, 2013).
Melanomas are thankfully uncommon, but do occur sporadically; prognosis is ominous (Ob. Gyn. 116: 1358, 2010).
![]() Melanoma of the vagina
Melanoma of the vagina
Pittsburgh Pathology Cases
ADENOCARCINOMA of the vagina arises from the glands of girls exposed to DES, usually in their teens. Fortunately, only one in about 1000 of girls exposed in this way get cancer, but the impact is devastating. The cells are glycogen-rich, hence the name "clear cell adenocarcinoma". This resembles its counterpart in the ovary.
EMBRYONAL RHABDOMYOSARCOMA, in its form of "sarcoma botryoides", is a common cancer of young children.
* There are many other rare tumors. Don't worry about these just now.
Remember the lymphatic drainage. Cancer in the lower two-thirds of the vagina metastasizes to the inguinal lymph nodes. Cancer of the upper third metastasizes to the iliac nodes.
{08914} normal histology of uterine cervix (endocervix is left, ectocervix is right)
{10271} normal ectocervix histology
{10274} normal endocervix histology
{36059} normal endocervical cells, pap smear
|
|
|
![]() Cervix
Cervix
"Pathology Outlines"
Nat Pernick MD
INFLAMMATION
Obviously herpes![]() ,
gonorrhea, and chlamydia will produce inflammation.
Especially if you see a lot of
lymphocytes with germinal centers, think of chlamydia.
,
gonorrhea, and chlamydia will produce inflammation.
Especially if you see a lot of
lymphocytes with germinal centers, think of chlamydia.
NON-TUMORS
MUCOPURULENT CERVICITIS may be caused by gonorrhea, or chlamydia, or grow nothing, and may or may not respond to antibiotics. Nobody understands it.
ENDOCERVICAL FIBROEPITHELIAL POLYPS are fibrous nubbins covered with epithelium, hanging out of the cervical os. They act as a wick, drawing bacteria into the endocervix and endometrial cavity. They are easily cured with curettage.
MICROGLANDULAR HYPERPLASIA results from progesterone stimulation of the endocervix (i.e., pregnancy, old-fashioned contraceptive pills). The glands are abundant and have only a lacy stroma between them, along with many neutrophils.
|
|
|
|
|
{09755} normal cervical pap smear (do you know the cell types?)
Worldwide, cancer of the cervix is the #2 cancer killer of women, second only to breast cancer. Often women die during their reproductive life. There are about 190,000 deaths worldwide each year (Am. J. Ob. Gyn. 189(s4): S37, 2003). In some of the poor nations, it is still the #1 cancer killer of women.
In the US, there are presently around 10,000 new cases of invasive cancer yearly, and almost 4000 deaths. The elderly, the poor, and especially those who are not routinely screened are by far the most common victims (Cancer 101: 1051, 2004).
In the US, the pap smear technique has greatly reduced a woman's risk of dying of the disease; as recently as the 1950's, it was as common a killer of Americans as breast cancer is today.
"Low grade SIL" (squamous intraepithelial lesion) usually corresponds to mild dysplasia / CIN I, or a flat or exophyic condyloma. "High grade SIL" usually corresponds to moderate/severe dysplasia (CIN II/III) or carcinoma in situ.
Fun to know: The average is around 10,000 cells on a routine pap smear, and the acceptable minimum is 5000 on one of the newer liquid thin-prep smears.
The vast majority (more than 80%) of cancers of the cervix are squamous cell carcinomas caused by HPV. Long before HPV was understood, we knew cancer of the cervix to be a sexually transmitted disease, with the great risk factors being the number of male sexual partners, and the number of previous female partners that the husband had. Update on HPV and cervical cancer: Lancet 370: 890, 2007.
Other possible risk factor include smoking (still discussed: JAMA 285: 2995, 2001; "and passive smoke exposure is an important independent risk factor" Am. J. Ob. Gyn. 204: 213, 2011 -- -- did we miss a coufounding variable?) and having an uncircumcised husband (seems to be due to circumcision protecting him from HPV; well-established by now).
The virulence factor is the E6 and E7 oncogenes, which differ for low-risk and high-risk HPV strains. (See Am. J. Path. 153: 1741, 1998; Cancer 83: 2346, 1998; lots more since. These bind p53 and Rb gene products. Finding a virulence factor is proof of causation -- it has replaced Koch's / Henle's postulates.)
Update on HPV and cancer of the cervix: Lancet 370: 890, 2007. Around 1 infected woman in 10 will get at least premalignancy.
DYSPLASIA OF THE CERVIX ("cervical intraepithelial neoplasia", today "cervical intraepithelial lesion") can exist for years or decades before invasive squamous cancer happens. (And of course, usually it never happens. But nobody wants to leave these lesions alone.) Or it can progress very rapidly.
CIN II: Plenty of atypical cells in the lower portions, normal maturation toward the surface. (The old "moderate dysplasia" and "severe dysplasia").
Worth knowing in today's cost-conscious era: The HPV-antigen L1 (one of those in the vaccine) is expressed in early HPV-related lesions; when a dysplasia LOSES L1 expression, it's likely to progress (why?) Update Am. J. Clin. Path. 132: 840, 2009.
CIN III: The cells no longer mature as they reach the surface. (The old "carcinoma in situ").
|
|
![]() Mild dysplasia
Mild dysplasia
HPV effect
Wikimedia Commons
{08911} uterine cervix, carcinoma in situ, histology
{08912} uterine cervix, carcinoma in situ, histology
{46209} cervical conization specimen. One may cure
CIS by removing the entire ring of abnormal cells.
* A huge variety of immunostains are coming into use for cervical intraepithelial lesions as prognosticators (Am. J. Clin. Path. 135: 212 & 253, 2011; Am. J. Path. 177: 884, 2010; Am. J. Ob. Gyn. 204: 21, 2011)
INVASIVE CANCER arising in from CIN III is usually squamous.
* There are some less common cancers, also:
![]() Squamous CA of the cervix
Squamous CA of the cervix
Pap smear
Wikimedia Commons
It is not always clear whether microinvasion has taken place, and today's hard-core pathologists use double immunostaining for keratin (the cancer cells) and collagen IV and/or laminin (for basement membrane). See Arch. Path. Lab. Med. 129: 747, 2005.
Surprisingly, there's no consensus about what lymph node is most likely to receive the first metastasis ("sentinel node") in cancer of the cervix. The best bet is "somewhere in the external iliac, obturator, or parametrial regions." Am. J. Ob. Gyn. 197: 678.e1-7, 2007.
* Surgery for advanced (even locally advanced) cancer of the cervix often includes removal of the bladder, rectum, or both. This still seems the best way to save lives (Am. J. Ob. Gyn 205: 148, 2011). You may hear the terms "North American", "South American", and "all-American" for these surgeries; it's cruel but the disease itself is more cruel.
Future pathologists: Staining pap smears routinely for p16INK 4a (or just p16 for short), which is an oncoprotein strongly overexpressed in premalignant / malignant cervical epithelial cells, may soon be routine as a way to help screeners. Though not specific, it seems 98% sensitive in picking up high-grade lesions (Cancer 105: 461, 2005). It's a surrogate marker for the HPV oncogenes being busy -- it's trying to counter them and is thus paradoxically overexpressed. Follow-up, using p16 and Ki-67, shows they greatly reduce the number of "don't know" pap smears (Arch. Path. Lab. Med. 131: 1343, 2007). Or a combination of p16 (stains nuclei red) and Ki-67 (proliferation marker, stains cytoplasm brown) when together are quite sensitive and specific for troublesome squamous and glandular lesions (Am. J. Clin. Path. 138: 625, 2012). The new antigen for staining is ProExC; along with p16, this seems specific for high-grade "CIN" (Am. J. Clin. Path. 135: 212, 2011).
It is uncommon, but not unheard-of, for a woman to present with an invasive squamous cell carcinoma despite having had regular pap smears / HPV assays that show no pathology (Arch. Path. Lab. Med. 136: 1533, 2012).
* Future pathologists: It is quite common for a cervical conization intended to fully remove a previously-diagnosed high-grade dysplasia to show no dysplasia, even after deep sectioning and p16 staining and a confirmation that the previous material did show disease. These patients need to be followed as the dysplasia may have been missed by the surgeon (Am. J. Clin. Path. 139: 422, 2013).
Juan Peron's previous wife had also died of cancer of the cervix. Pap smears were in use in the developed world in the late 1940's, but had not caught on in Argentina. In January 1950, Ms. Peron fainted in public and was found to be anemic, evidently as the result of iron deficiency from blood loss due to her cancer. It's not clear whether her cancer was found at the time, but she continued to have heavy vaginal bleeding. She was taken to surgery and operated by an American "ghost surgeon"; she was never informed of what had been done, who operated her, or the nature of her illnesss. How much of this was the "fifties" mentality ("beneficience" / "paternalism" / "the duty NOT to tell a cancer patient the diagnosis" / the general concealing of unpleasant truths)? How much was the "VIP syndrome", in which prominent people get their health problems concealed from the public? You'll have to decide this for yourself. Ms. Peron was enormously popular with her people, especially for her advocacy for the poor. She was one of the most beautiful and charismatic women of her era -- perhaps any era. My reading tells me that most of today's historians consider her a genuine humanitarian. You can read about her final illness in Lancet 355: 1988, 2000. |
 Evita |
* Future pathologists only: To determine whether an adenocarcinoma here is of endometrial or endocervical origin, stain for estrogen receptor and vimentin (both positive in most endometrial adenocarcinomas and negative in most endocervical carcinomas), and p16 and CEA (both positive in most endocervical adenocarciomas and negative in most endometrial carcinomas.)
* Leave the diagnosis of the rare very-low-grade "adenoma malignum of the endocervix" to us. Loss of PAX2 is a tipoff.
Of course, squamous cell carcinoma and adenocarcinoma occur together fairly often (Cancer 102: 218, 2004). Complying with recommendations for routine pap smears greatly decreases, but does not eliminate, a woman's risk for this cancer (Cancer 99: 336, 2003).
Medical school undergraduates do not really need to learn to read pap smears, but it's enriching. The old-fashioned pap smear (you smear the specimen on a slide) includes more cells than the newfangled "liquid thin prep" (you put the specimen in fixative; easier to read Cancer 99: 342, 2003; won't see tumor diathesis as on a classic pap smear), despite early claims (Br. Med. J. 326: 733, 2003) it's really neither better nor worse in terms of sensitivity or specificity compared to the ordinary old smears (Ob. Gyn. 111: 167, 2008; Ob. Gyn. 112: 1327, 2008). Computers ("Auto-Pap"/"Focalpoint") now screen pap smears with accuracy about equal to a human cytotechnologist (Cancer 99: 129, 2003). And even experienced pathologists do not always make the right call on either type of test: Arch. Path. Lab. Med. 127: 1413, 2003; Arch. Path. Lab. Med. 128: 17, 2004). If a pap smear that you obtained on one of your patients does not include any endocervical cells (columnar or squamous-metaplastic, we can tell), we'll let you know that you probably did not sample the "transformation zone", where ectocervix joins endocervix and most dysplasia / carcinoma-in-situ and invasive cancers begin. And of course, there are both squamous and glandular cells that look just a little bit strange ("litigation cells"), and no one knows what they mean (Ob. Gyn. 107: 701, 2006).
The "atypical glandular cell", which may be the precursor of, or the only sign of the early presence of, either cervical or endometrial adenocarcinoma, is especially difficult -- women with high-risk HPV are likely to have cervical cancer, those without endometrial cancer (no surprise) (Ob. Gyn. 115: 243, 2010; Arch. Path. Lab. Med. 134: 103, 2010).
Your lecturer predicted in 2003 that the routine pap smear would soon be supplemented in most cases by routine DNA probing for the high-risk HPV strains, with pap smear/biopsy limited to those who are positive. See Arch. Path. Lab. Med. 127: 940 & 969 & 984 & 991 & 995, 2003; Arch. Path. Lab. Med. 128: 298, 2004; Postgrad. Med. 118: 37, 2005. It's now clear that pap smears miss about a quarter of patients with high-risk HPV infection and (?) smoldering premalignancy: Cancer 111: 1, 2007. Women with high-grade dysplasia or invasive cancer apparently ALL test positive for HPV: Am. J. Ob. Gyn. 189: 118, 2003. It is now clear that this does indeed reduce the rate of high-grade lesions in the upcoming years; expect it to be standard soon, perhaps even replacing the routine pap smear (NEJM 357: 1579 & 1589, 2007).
Also watch special staining of pap smears for markers of proliferation (notablyProEx C and the more-familiar MIB-1: Cancer 114: 196, 2008). They seem to correlate with how mean an intra-epithelial lesion is, supplementing information from the appearance of the cells.
* Almost all invasive cervical cancers have amplified TERC, the human telomerase gene. The Swedes have developed FISH to look for amplified TERC on pap smears, and of course find that the ones with amplified telomerase are much more likely to harbor aggressive lesions. I doubt this will become clinically useful, since the women are going to get biopsied anyway, but it's interesting (Am. J. Path. 175: 1831, 2009).
The HPV vaccine ("Gardasil"): NEJM 356: 1915 & 1928, 2007; J. Inf. Dis. 196: 1438, 2007. The latter reports that the quadrivalent gives essentially complete protection against HPV-6, -11, -16, and -18 so long as she has not yet met that particular strain. It's an expensive and painful injection.
The popular explanation (put forward in For. Sci. Int. 87: 219, 1997) is that she had taken the quack cancer remedy dimethylsulfoxide (DMSO), and that it gave rise to the poison gas dimethyl sulfate.
Is this credible?
Yes!
No!
* In the monster movie Godzilla 2000, a photomicrograph of the monster's skin is examined by a group of scientists. Fascinatingly, it appears identical to normal human ectocervix.
|
|
|
|
|
|
|
|
|
|
|
INTRODUCTION
|
|
Following deliveries, the uterus may prolapse.
Words to know:
Leave the dating of endometrial samples to pathologists. You will usually get one of these diagnoses:
The endometrium is very resistant to bacterial infection.
Infection by common bacteria (strep A![]() ,
staph
,
staph![]() )
is usually the
result of retained products of conception. Surgical removal of
the remnants
is the mainstay of therapy.
)
is usually the
result of retained products of conception. Surgical removal of
the remnants
is the mainstay of therapy.
Pyometra is thankfully rare. It is a purulent infection of the uterus, as when products of conception are retained or the os is closed.
Other infections after childbirth or natural or induced
abortion include strep![]() ,
staph
,
staph![]() ,
and E. coli. In the Bad Old Days before
common-sense hygiene, physicians carried these infections from woman to woman
on the delivery unit.
,
and E. coli. In the Bad Old Days before
common-sense hygiene, physicians carried these infections from woman to woman
on the delivery unit.
![]() On the Coontagiousness
On the Coontagiousness
of Puerperal Fever
Oliver Wendell Holmes MD
Acute endometritis (i.e., neutrophils well before menstruation) often has no obvious cause; various mycoplasma are the "usual suspects" and this is now being confirmed with PCR: Lancet 359: 765, 2002
Chronic endometritis was once defined to be the presence of plasma cells in the endometrium -- since no one really knows what the clinical picture is, there's probably no better definition. Usually this is the result of gonococci or chlamydia having their home base in the oviducts (confirmed by response to therapy: Am. J. Ob. Gyn. 190: 305, 2004), or else simply the effect of compression by a nearby leiomyoma (nobody knows how).
* There seems to be only a minor or no correlation with bacterial vaginosis (Am. J. Ob. Gyn. 195: 1611, 2006).
Less often, retained products of conception are the cause. Obviously an intrauterine contraceptive device will produce chronic inflammation.
Also remember TB![]() , especially in the poor nations.
, especially in the poor nations.
Thankfully, nobody still uses the magnesium-rich super-absorbent tampons
that proved such a good culture medium for the
staphylococci![]() that
produce toxic shock syndrome.
that
produce toxic shock syndrome.
|
|
ADENOMYOSIS ("endometriosis interna")
It's easy to tell this isn't cancer, since the glands are benign and there is stroma with them.
A common criterion for diagnosis is glands-plus-stroma one medium-power field width below the endometrial-muscular junction. However, pathologists differ widely in whether they "call" it. One recent study (which suggested that previous instrumentation can be a cause, which makes sense) found about half of uteruses removed for whatever reason to contain at least "pathologist's adenomyosis" (Ob. Gyn. 104: 1034, 2004 -- even more common than the standard "one uterus out of five has incidental adenomyosis"). Obviously this can cause discomfort just before and during menstruation. You'll be told that adenomyosis is one of the major causes of menstrual cramps, and there is no question that some women with adenomyosis have no other clear cause and do get relief from hysterectomy. Irregular bleeding is also attributed to the process.
An adenomyoma is a nodule where there is a great deal of adenomyosis. More often, the process is diffuse, and if severe will expand the uterus.
* Contrary to old work, at least new studies confirm that adenomyosis lesions do in fact contain progesterone receptors (Gyn. Ob. Inv. 45: 126, 1998; Eur. J. Gyn. Onc. 254: 222, 2004).
{14330} adenomyosis, histology
![]() Adenomyosis
Adenomyosis
Text and photomicrographs. Nice.
Human Pathology Digital Image Gallery
ENDOMETRIOSIS ("endometriosis externa", BMJ 334: 249, 2007)
Don't worry about the etiology. The various ideas ("regurgitation", i.e., retrograde menstruation; metaplasia of the coelomic epithelium; metastases via lymphatics) all probably operate at different times.
* Your lecturer is watching new claims about mutations in endometriosis with some interest. Old reports of mutations came from studies of already-established cell cultures, that might have been immortalized by mutations after being obtained from the patient.
Being on the oral contraceptive pill seems to prevent endometriosis from forming.
At least one women in 10 will have symptoms of endometriosis during reproductive life. Endometriosis cycles like endometrium does.
The gross appearance of endometriosis depends on how extensive the disease is.
Longstanding ovarian lesions present "chocolate cysts", full of old blood.
Large lesions where the blood has organized present extensive fibrosis. This can obliterate the pouch of Douglas, obstruct the bowel, obstruct the oviduct, and so forth.
Understandably, these lesions can produce dyspareunia (pain on intercourse), constipation, and dysmenorrhea (pain on menstruation).
Endometriosis is a clear risk factor for two types of ovarian cancer (clear-cell and endometrioid). These tumors tend to bear mutant and/or lost ARID1A / BAF250a (NEJM 363: 1532, 2010); and the BAF250a gene is often lost in benign endometriosis (In. J. Clin. Exp. Path. 5: 642, 2012).
Infertility often accompanies endometriosis; exactly how this happens is a minor mystery.
![]() Endometriosis of Ovary
Endometriosis of Ovary
Text and photomicrographs. Nice.
Human Pathology Digital Image Gallery
ENDOMETRIAL POLYPS
The histology may seem normal, or show some cystic hyperplasia (see below). The tipoff that curettings contain a polyp is the presence of thick-walled blood vessels (i.e., they've had time to develop and not been shed every month.) Removal by curettage usually is curative.
With today's imaging, we are picking up lots of "polyps" that aren't bleeding, and there's always the question of "Which ones need to be removed?" An older woman (peri-menopausal or post-menopausal), especially if hypertensive, probably needs it excised, as there's a fair risk that it's not a real polyp, but a pre-cancer or cancer (Am. J. Ob. Gyn. 201: 462.e1, 2009).
ENDOMETRIAL HYPERPLASIA / "ENDOMETRIAL INTRAEPITHELIAL NEOPLASIA"
Nobody really knows the "risk of turning into adenocarcinoma", since the diagnosis is made only on biopsy and this itself affects the illness (curettage may be curative).
Hyperplasia, and its distinction from well-differentiated adenocarcinoma, is still best called on cyto-architecture rather than cytologic features (Cancer 108: 77, 2006). That sounds easy and the World Health Organization made a standard in 2003, but reproducibility of diagnosis is poor, even among subspecialist pathologists (Cancer 106: 804, 2006). Soon we may be making calls on molecular markers (Am. J. Ob. Gyn. 204: 357.e1-12, 2011; Am. J. Clin. Path. 138: 678, 2012.)
SIMPLE HYPERPLASIA ("cystic hyperplasia", "mild hyperplasia", "endometrial hyperplasia without atypia") features:
|
|
Not everyone likes the current (WHO) system, and some pathologists are distinguishing "atypical hyperplasia" and the supposedly-meaner "endometral intraepithelial neoplasia". The requirement is crowded glands presenting an area greater than stroma, with the cells different in morphology from the cells in the nearby normal endometrium ("cytologic alteration"); there are some immunostains that are somewhat helpful (Am. J. Clin. Path. 138: 678, 2012). Be this as it may, one big study reports that prognosis seems to be the same (Cancer 113: 2073, 2008).
Other pathologists distinguish BENIGN ENDOMETRIAL HYPERPLASIA ("to be managed with hormonal treatment") to involve all of the endometrium, and ENDOMETRIAL INTRAEPITHALIAL NEOPLASIA ("to be managed surgically unless she very much wants to have a child") to be a focal area that is clearly more disturbing than the rest. If there are cribriform areas, solid areas, bridges, or mazes, it's adenocarcinoma instead. Stay tuned.
ENDOMETRIAL ADENOCARCINOMA
Most of these are "type I endometrial adenocarcinomas." The risk factors are well-known.
Also remember
Patients present with bleeding because of the invasion of the inner wall. Thankfully, these tumors usually announce themselves early. Only about one woman in six with cancer of the endometrium will die from it.
Grossly, the lesions look like cottage cheese.
Microscopically, in the common "endometrioid adenocarcinoma" (about 80% of these cancers) the pathologist sees back-to-back glands and/or a dense stroma between glands with nuclear atypia. Solid sheets of cells are more ominous. This has been general knowledge for decades and was recently reconfirmed in Am. J. Clin. Path. 129: 110, 2008. The grading system for endometrioid cancer:
Increase the grade by one if the nuclei are unusually ugly.
By no means are the G1's particularly tame. Around 15% of them will spread beyond the uterus (Am. J. Ob. Gyn. 198: 216.e1-5, 2008).
* The genetic mutations that drive type I endometrial adenocarcioma are often in beta-catenin, k-ras and the mismatch repair proteins.
* Soon we may be prognosticating endometrial adenocarcinomas on the molecular marker expression. The combination of survivin, p21, and p53 seems to be the best predictor of aggressiveness (Am. J. Ob. Gyn. 200: 78e1, 2009).
If there is benign-looking squamous metaplasia, the pathologist describes "endometrial adenocarcinoma with squamous metaplasia" (* formerly "adenoacanthoma"). This is of little significance.
If there are squamous areas and they are anaplastic, the pathologist describes "adenosquamous carcinoma". This tends to be aggressive.
Metastases eventually can occur, usually via the lymphatics.
SEROUS ADENOCARCINOMA OF THE ENDOMETRIUM ("* type II uterine epithelial carcinoma"; Cancer 101: 2214, 2004; Cancer 104: 1391, 2005 -- HER2/neu amplification and all that this implies) and CLEAR CELL CARCINOMA OF THE ENDOMETRIUM are more aggressive, look like the corresponding ovarian lesions, and are less likely to be linked to high estrogen or to previous hyperplasia.
* The precursor lesion of endometrial serous carcinoma is overexpressed p53, even when the endometrium looks normal (Am. J. Path. 174: 2000, 2009).
* As elsewhere, HER-2/neu amplification is a strong predictor of bad outcome in the papillary serous lesion (Cancer 104: 1391, 2005). Watch for herceptin as an agent to treat these patients.
* Let us make the distinction, especially between the tamer "endometrioid" cancer and the more aggressive ("always grade 3") serous cancer. The latter will light up with IMP3 (Am. J. Clin. Path. 133: 899, 2010).
* Future pathologists only: Papillary serous tumor primary in the endometrium will stain negative with WT1; papillary serious carcinoma primary in the ovary will stain positive with WT1.
* Service pathologists often make mistakes here. Update Arch. Path. Lab. Med. 137: 1574, 2013.
* UNDIFFERENTIATED ENDOMETRIOID CARCINOMA: Again, let us worry about this. Am. J. Clin. Path. 137: 438, 2013.
|
|
|
|
MIXED MULLERIAN / MESENCHYMAL TUMORS
There is often a history of previous radiation (radiation-associated endometrial carcinoma is often histologically bizarre and tends to be more aggressive than ordinary endometrial carcinomas: Ob. Gyn. 113: 319, 2009).
They tend to be aggressive and to metastasize as adenocarcinomas.
The tendency nowadays is to call them "endometrial adenocarcinomas with sarcomatous metaplasia."
* ENDOMETRIAL STROMAL TUMORS are of three types. Leave the diagnosis to us; their histology is not for medical school undergrads.
Pathologists need special stains to tell these from spindle cell tumors of smooth muscle origin. Muscle tends to light up with caldesmon; endometrial stromal cells tend to light up with CD10 and B-catenin, but there is overlap.
![]() Endometrial Stromal Sarcoma
Endometrial Stromal Sarcoma
Text and photomicrographs. Nice.
Human Pathology Digital Image Gallery
LEIOMYOMAS (Lancet 357: 293, 2001; Ob. Gyn. 104: 393, 2004; NEJM 372: 1646, 2015)
The etiology is mysterious. They grow in response to estrogen and (we recently discovered) also require progesterone (Endocrinology 151: 2433, 2010), and shrink (and often vanish) after menopause.
* Multiple chromosome breaks and reassembly seems to be the common genetic theme: NEJM 369: 43, 2013.
Usually leiomyomas are asymptomatic, or cause problems by mass effect. A submucosal leiomyoma can produce bleeding between periods, and interfere with fertility. Large leiomyomas can cause problems with pregnancy.
The tumors are rubbery white spheres. Grossly, the "whorled silk" pattern seen on cross-section is famous.
Tumors may calcify, show central necrosis (watershed infarct; when this becomes infected it's a "pyomyoma" -- think staph, strep, and now salmonella Ob. Gyn. 116(S2): 291, 2010), and/or fatty ingrowth. A few pathologists distinguish a "cellular leiomyoma" (with very little fibrous stroma) from the more familiar type with more collagen (Am. J. Ob. Gyn. 203: 109, 2010).
The new procedure of embolizing these tumors under fluoroscopy, rather than removing the uterus, seems safe and effective (Am. J. Ob. Gyn. 190: 1697, 2004; Ob. Gyn. 106: 52 & 1309, 2005; AJR 184: 399, 2005). The most serious risk is infection in the necrotic debris (OB Gyn 104: 1161, 2004). And prior to surgery, leiomyomas may be shrunk using a GNRH antagonist (BJOG 112: 638, 2005). Anastrazole (the aromatase inhibitor) for leiomyomas: Ob. Gyn. 110: 643, 2007.
{08438} leiomyoma of uterus, gross
{09774} leiomyoma of uterus, gross
{10910} leiomyoma of uterus, gross
{24703} leiomyoma of uterus, gross
{39636} leiomyoma of uterus, gross
{49380} leiomyoma of uterus, gross
{08728} leiomyoma, histology
{08729} leiomyoma, histology
{49383} lipoleiomyoma
{20184} calcified uterine leiomyomas, radiograph
|
|
|
|
INTRAVASCULAR LEIOMYOMATOSIS means a bunch of leiomyomas with a proclivity to grow down the veins. Curiously, this doesn't metastasize, and regresses after menopause.
* The rare, oxymoronic "benign metastasizing leiomyoma / leiomyomatosis of the lung" is perhaps the least aggressive of all sarcomas. The tumors pop up in the lungs (Am. J. Med. Sci. 338: 72, 2009; Ann. Thor. Surg. 93: e149, 2012). "Wait-and-see" is perhaps best (Ann. Thorac. Surg. 87: 613, 2009).
LEIOMYOSARCOMAS of the uterus are fairly common. If you see a smooth muscle tumor of the uterus that's grossly worrisome and has ten or more mitotic figures per ten high power fields, or if you see fewer with obvious anaplasia or cell necrosis, it's a leiomyosarcoma. (* "Two out of three, mitoses, anaplasia, necrosis" may be the rule today; the benign nature of the "mitotically active leiomyoma" has been recognized for two decades -- Am. J. Clin. Path. 97: 14, 1992. Leave the tough ones up to us.) Prognosis depends on the histology -- some pathologists call a tumor with mitotic figures but not enough anaplasia or necrosis "smooth muscle tumor of uncertain malignant potential." A tumor less than 5 cm is unlikely to be a leiomyosarcoma. The whole business is being reshuffled right now -- update Arch. Path. Lab. Med. 132: 595, 2008.
|
|
PELVIC INFLAMMATORY DISEASE ("salpingitis"): NEJM 372: 2039, 2015.
Actinomycosis![]() usually results from the presence of an intrauterine
device, on which the "superglue bug" can build its "sulfur granules"
colonies.
usually results from the presence of an intrauterine
device, on which the "superglue bug" can build its "sulfur granules"
colonies.
Gonococcal and chlamydial "PID" is a sexually transmitted disease, and unfortunately very common. It can smolder, with pain being worst during the menstrual periods. During acute flareups, there is severe pelvic pain, especially when the cervix is manipulated, with peritoneal signs.
Grossly, the tubes are swollen and inflamed. They may be packed with pus ("pyosalpinx"). During the acute phase, the pathologist will see neutrophils and marked edema. In chronic infection, there is a mix of neutrophils, lymphocytes, and other inflammatory cells. After everything is over, there is likely to be a lot of scarring, which will probably interfere with fertility; if the ends of the tubes are plugged by scar tissue, a "hydrosalpinx" results.
Women still die of PID, either in the acute phase (sepsis) or from complications (peritonitis, obstruction).
* How much "unexplained infertility" in women is due to subclinical / inadequately treated pelvic inflammatory disease has always been an unanswered question. It's probably fairly high (Ob. Gyn. 120: 37, 2012).
* Tubal infections that follow abortion or a childbirth infection tend to involve the mucosal surfaces rather than the lumen.
OTHER LESIONS OF THE OVIDUCT
CYSTS arise from embryonic structures. Hyatids of Morgagni / paratubal cysts arise from mullerian duct remnants and are mere curiosities.
A patient with old pelvic inflammatory disease may be told that her dilated, fluid-filled oviducst are "cysts".
Adenocarcinoma of the oviduct is very rare and very deadly. Adenomatoid tumors are hard white spheres that arise from mesothelium.
We will cover ECTOPIC PREGNANCY below.
A HERMAPHRODITE is defined to possess at least some ovarian and some testicular tumor. This is very uncommon, and you'll learn how it can happen in your embryology course.
You are already familiar with the "streak ovaries" of Turner's 45 XO.
* Are there perhaps normally more than one ovulation per month? Br. Med. J. 327: 124, 2003.
|
|
|
|
|
|
![]()
{24817} normal ovary in pregnancy
{24695} normal graafian follicle
{24696} normal graafian follicle, higher power
{24698} radiation injury to ovary; note loss of germ cells and radiation change in vessels
* One animal model involves autoimmunization with zona pellucida (ZP3): Mol. Rep. Dev. 48: 140, 1997 -- watch this antigen, as it's being discussed as a reversible contraceptive. Curiously, some mice develop autoimmune oophoritis after thymectomy.
PRIMARY OVARIAN FAILURE, defined to be arrest of normal function before age 40, happens in 1% of women. It is often familial.
OVARIAN TORSION usually is caused by an ovarian mass, but can happen at any age.
* Treating it in the unborn (!) -- J. Ped. Surg. 32: 1447, 1997.
![]() Ovary with torsion, gross
Ovary with torsion, gross
WebPath
The mysterious "massive ovarian edema" might be the result of partial torsion (J. Rep. Med. 41: 359, 1996) or (seems more likely to me) thrombosis of the ovarian vein.
CYSTIC FOLLICLES ("follicular and luteal cysts")
{00105} cystic follicles in ovary
Big ones can cause torsion and/or possess too much luteinized theca cell tissue resulting in hyperestrogenism.
CORPUS LUTEUM CYSTS are simply oversized. They are filled with blood and fatty debris, so when a corpus luteum cyst undergoes torsion or ruptures, it's a bit more of a problem.
STEIN-LEVENTHAL SYNDROME ("polycystic ovarian disease / syndrome"; Lancet 370: 685, 2007)
We used to think "the fibrosis around the ovary prevents ovulation." The worst enemy of wrong hypotheses is facts, and it's now known that around 25% of normal women during reproductive life have polycystic ovarian morphology (J. Clin. Endo. Metab. 91: 3878, 2006), and the vast majority never have any problems.
And of course, ovaries with numerous cysts but lacking the outside fibrosis have nothing to do with Stein-Leventhal.
* A consensus conference in 2003 came up with the "Rotterdam Criteria" for scientists; they're under review as too narrow, and there are a host of sub-phenotypes (Am. J. Ob. Gyn. 198: 670e, 2008; BJOG 116: 1633, 2009). In a nutshell, two of three without any other obvious casue: (1) at least one ovary with 12 or more cysts 2-9 mm and/or a total volme of 10 mL or more; (2) clinical or biochemical signs of hyperandrogenism; (3) oligo- or anovulation.
Obese young women with polycystic overy syndrome tend to have much worse coronary atherosclerosis than their normal peers: J. Clin. Endo. Metab. 92: 4609, 2007.
The failure of ovulation results from no follicle becoming dominant, or reaching the full size for ovulation (J. Clin. End. Metab. 83: 3984, 1998). Since nobody knows how one follicle comes to be selected as dominant, our understanding of Stein-Leventhal is probably a long way off.
Biopsies obtained during laparotomy shows that women with polycystic ovary disease, even when mild and the woman is still ovulating, have much more early-growing follicles than do normal women (Lancet 362: 1017, 2003).
Because androstenedione can turn into estrone, hyperestrogenism can also be a problem, including risk for endometrial adenocarcinoma.
Your lecturer suspects that the principal cause is some hormone awaiting discovery.
The hormonal symphony (or cacophony) include leptin, its receptor, adiponectin (down, early), insulin (up from resistance), testoserone (up), adrenal androgens (up), triglycerides (up) "omentin-1, a novel adipokine" (down; ever heard of that one? Diabetes 57: 801, 2008), and a host of others (J. Clin. Endo. Metab. 92: 2659, 4637 and 4771, 2007). Especially if there is hyperandrogenism, the liver is likely to become fatty independent of obesity and insulin resistance (J. Clin. Endo. Metab. 97: 3709, 2012)
And within the ovary, both theca and granulosa cells overexpress / underexpress a host of genes (J. Clin. Endo. Metab. 93: 4456, 2008).
Perhaps the cysts form because the granulosa cells themselves proliferate instead of dying as they should at the end of the month: J. Clin. Endo. Metab. 93: 881, 2008).
The disorder is obviously polygenic and probably environmentally-related.
I predicted a link to metabolic syndrome X and non-alcoholic steatohepatitis in the 1980's; this is now amply supported (Med. J. Aust. 174: 580, 2001 first, now J. Clin. Endo. Metab. 91: 1741 & 2789, 2006).
* Currently, metformin seems to work well to control Stein-Leventhal (Br. Med. J. 327: 951 & 974, 2003), along with diet and exercise of course. Proglitazide: J. Clin. Endo. Metab. 93: 3618, 2008. Stay tuned.
STROMAL HYPERTHECOSIS ("cortical hyperthecosis") features hyperplasia and luteinization of the theca cells, making them overproduce androstenedione. The ovaries are big and yellow. Most (but not all) patients are post-menopausal.
|
INTRODUCING THE OVARIAN TUMORS (research pathologists see Am. J. Path. 177: 1053, 2010)
|
|
Screening for these tumors to prevent cancer deaths has been a failure. Even the combination of blood CA-125 (produced by most serous and endometrioid ovarian cancers) and transvaginal ultrasonography did not prevent deaths from ovarian cancer (JAMA 305: 2295, 2011).
There are three overriding categories of ovarian tumors.
They are rare before age 30.
Sometimes a benign one will be almost all stroma, and be called an "adenofibroma".
Any of these can also be primary on the peritoneum.
Since the coelomic epithelium is continuous across both ovaries, and since cancer arises in a mutated field, the malignant ones tend to be bilateral when diagnosed; this does not make them incurable.
The malignant ones tend to metastasize over the peritoneum and cause death by obstructing the bowel. These are the common ovarian cancers.
Lynch's hereditary colon polyposis (HNPCC) also puts a woman at increased risk (JAMA 277: 915, 1997, much-confirmed by now).
Time on the oral contraceptive pill, or time pregnant, is protective apparently regardless of hereditary risk. Perhaps ovulation gives the coelomic cell the opportunity to divide which allows selection for the mutated clones. Despite the perennial talk about the very real health risks of the oral contraceptive pill, today's estimate is that it prevents 30,000 ovarian cancers, and 15,000 deaths from ovarian cancer, annually (Lancet 371: 303, 2008).
Update for pathologists on ovarian cancer: Arch. Path. Lab. Med. 133: 1775, 2009.
For some reason, tubal ligation seems to protect somewhat; despite a hoopla some years back, fertility drugs don't seem to be a risk (Mayo Clin. Proc. 82: 751, 2007).
* Not so long ago there was a hoopla about cornstarch and talcum powder applied to the perineum as causing ovarian cancer. This makes no sense biologically, and it sounds like recall bias explains the early reports. Of course it was amply refuted (Am. J. Ob. Gyn. 182: 720, 2000). It's now back... one patient with pelvic lymph node talcosis had ovarian cancer (Ob. Gyn. 110: 498, 2007). I'll take this seriously when there are controls.
They can occur at any age. They are almost always unilateral.
* There is an autosomal dominant tumor syndrome at DICER1, involved in processing microRNAs (NEJM 366: 234, 2012).
* Future pathologists: They light up with inhibin.
They usually occur in children and young women.
The most common is the benign, banal dermoid tumor ("cystic teratoma") of young women. The other common ones are all cancers; the younger the patient, the more likely to be malignant.
METASTASES TO THE OVARY are common, especially from breast and stomach. The latter especially is a common presentation for stomach cancer, the infamous "Krukenberg tumors" with massive bilateral enlargement of the ovaries, which prove at surgery to be stuffed with signet ring cells (update Arch. Path. Lab. Med. 130: 1725, 2006).
Most of these are malignant; a majority of the malignant ones arise bilaterally. This is the single most common ovarian cancer (about 40%).
Benign serous tumors are quite tame-looking and always have a lot of cilia. Surgery is curative.
![]() Ovarian serous cystadenoma
Ovarian serous cystadenoma
WebPath
Borderline tumors have piling-up of the cells (to three layers), perhaps with some anaplasia but with no invasion of the stroma. Surgery is usually curative; if a borderline has metastasized (usually over the peritoneal surface), survival is still likely for years or decades.
When a serious ovarian tumor is fully-malignant, the fact that it's cancer is obvious.
Future pathologists:
* For some reason that no one understands, peritoneal mesothelioma is becoming so common in Japan that distinguishing it from ovarian cancer has forced pathologists to come up with a panel of immunostains. Calretinin and thrombomodulin stain mesotheliiomas. Ber-EP4, MOC-31, CA19-1, and estrogen receptor stain serous ovariain cancer (Am. J. Clin. Path. 130: 771, 2008). What's more disturbing about this paper is the epidemic of peritoneal mesothelioma itself. Watch this.
There are at least three different grading systems. Probably the best today is simply going "low-grade" (little anaplasia, few mitotic figures) versus "high-grade" (much anaplasia, many mitotic figures) (Cancer 118: 3087, 2012).
What will probably turn out to be just as important is the genotyping, worth learning now.
High-grade serous carcinoma usually has a p53 mutation early, without the k-ras or b-raf mutations.
|
|
Most of these are benign, with well-developed columnar cells and abundant mucin. They are always multicystic and can be very large. Benign mucinous tumors are very common. They are usually unilateral. Most of the tabloid newspaper tumors that weigh so much are benign mucinous cystadenomas.
|
|
Borderline tumors exhibit some stratification of nuclei and/or anaplasia (much as you'd see in a colon adenoma), but no invasion of the stroma. Again, surgery is usually curative, and metastatic disease is compatible with long survival.
![]() Borderline mucinous tumor
Borderline mucinous tumor
Ovary H&E
Wikimedia Commons
"Primary mucinous carcinoma of the ovary" is diagnosed much less often than in the past. Most of the older cases are now known to have been metastases; true primary mucinous carcinoma of the ovary is a relatively low-grade, not-very-aggressive, unilateral cancer; if you see mucin lakes or signet-rings, it's a metastasis.
* "Pseudomyxoma peritonei", in which mucin erupts into the peritoneal cavity and elicits a fibrous response, often results from mucinous carcinoma of the appendix; it is much less likely to result from an ovarian primary.
ENDOMETRIOID TUMOR (Cancer 112: 2211, 2008)
Pathologists recognize them by their resemblance to swiss-cheese endometrial adenocarcinoma.
The risk factors are the same as for endometrial adenocarcinoma; there is often a history of endometriosis in the ovary as well.
About half are bilateral. Often there is a coexisting endometrial carcinoma, but this does not imply that these are metastases; the diseases are still surgically curable.
Be this as it may, this tumor shows lots of big clear cells in sheets or tubes.
"Clear cell tumors" of the ovary are all malignant and tend to be aggressive. Endometriosis of the ovary is a significant risk factor. The hereditary risk syndromes for serous cancer seem not to give increased risk here; the genetics are distinctive -- the cancer genotype is stable (unlike serous carcinoma -- which is why the response to platinum chemotherapy is so poor -- J. Clin. Path. 60: 355, 2007; NEJM 363: 1572, 2010).
* A distinctive mutation present in around half of these (PIK3CA) might be a target for chemotherapy that actually works (Am. J. Path. 174: 1597, 2009).
* Speaking of this... the genetic mutations driving ovarian cancer are just now being worked out. Oncologists now describe "type I" ovarian cancers (no mutated TP53 or PIK3CA) and the more aggressive "type II" ovarian cancers (one or both mutated; Am. J. Path. 182: 1391, 2013.)
![]() Clear cell adenocarcinoma of the ovary
Clear cell adenocarcinoma of the ovary
Pittsburgh Pathology Cases
BRENNER TUMOR
They are almost all benign, and very little's written about them.
* An old claim that finding "transitional cell carcinoma-like areas" in metastatic ovarian cancer was a good prognostic indicator turned out not to work: Am. J. Clin. Path. 109: 173, 1998.
{27083} Brenner tumor, histology
{39859} Brenner tumor, gross
{40518} Brenner tumor, histology
![]() Brenner tumor
Brenner tumor
Tom Demark's Site
GERM CELL TUMORS (Am. J. Clin. Path. 109(S1): S82, 1998)
Contrary to "Big Robbins", the tissues of a teratoma look like those in the fetus or young baby, rather than in the adult. The hair is the most likely stuff to look mature.
About 15% are bilateral. All have the 46XX karyotype ("Mommy's girl"). Rarely a squamous cell carcinoma will arise in one of these (series BJOG 114: 1283, 2007), but otherwise they are thoroughly benign.
Occasionally, a teratoma will look enough like an unborn child to be identifiable as such. This is called a "homunculus" (Arch. Path. Lab. Med. 130: 1552, 2006 -- disturbing images).
The "growing teratoma syndrome" (first observed in men treated for testicular carcinoma) is recurrence of a clearly-malignant germ cell tumor after successful radiation and/or chemotherapy, as one or more masses that prove to be mature teratomas. It is also well-known in women following germ cell malignancies (Ob. Gyn. 108: 509, 2006); since they have more malignant potential than never-malignant teratomas, they should be removed.
![]() Ovarian Dermoid
Ovarian Dermoid
Dino Laporte's PathosWeb
SPECIALIZED TERATOMA ("monodermal teratoma", from one germ layer, actually a contradiction in terms)
"Gliomatosis peritonei" is peritoneal implants of glial tissue in girls with an immature teratoma. These seldom become frankly malignant, and no one really knows what to do about them (Br. J. Rad. 80: e101, 2007).
* Huge series of ovarian teratomas of all sorts from Korea: Am. J. Ob. Gyn. 205: 32.e1-4, 2011.
DYSGERMINOMA
Like seminomas, some produce hCG. Like seminomas, they are very sensitive to radiation and chemotherapy. They are quite common but are not much-studied nowadays -- thanks to their excellent response to treatment.
ENDODERMAL SINUS TUMOR ("yolk sac tumor")
Like the yolk sac, they are loaded with alpha-1 antitrypsin and alpha-fetoprotein.
Leave the identification of Schiller-Duval bodies, which recapitulate the duct of the yolk sac, to the pathologists.
These used to be uniformly lethal, but now most are cured with chemotherapy.
Miscellany
CHORIOCARCINOMA can be primary in the ovary; since this has none of Dad's tissue antigens for the immune system to reject, it's harder to cure than gestational trophoblastic disease.
* A primary ovarian choriocarcinoma with some of the husband's chromosomes: Ob. Gyn. 102: 991, 2003.
* A "polyembryoma" contains hundreds of little structures that look like developing embryos. Puzzle that one out!
* No one knows where to place "hypercalcemic small cell carcinoma of the ovary". It looks like oat-cell of the lung, behaves aggressively, and (2/3) causes hypercalcemia in young women.
This is the best name for tumors that contain abundant granulosa-type cells (cuboidal steroid-producing cells), often with some forming Call-Exner bodies (holes for eggs, as in the normal ovary).
There are often theca cells as well, and these may be spindly, or pink and plump (luteinized).
Many of these produce estrogen. A few produce androgen. As steroid-producers, expect yellow on the gross.
* A type that occurs in children and sometimes adults ("juvenile granulosa cell tumors") tends to be more anaplastic with sheets of cells and only an occasional follicle.
* Essentially all "adult-type" granulosa tumors seem to bear a trademark substitution in the FOXL2 gene (earliest known marker for ovarian differentiation; NEJM 360: 2719, 2009).
Any granulosa tumor can metastasize. It's also common for them to rupture, producing a hemoperitoneum.
THECOMA-FIBROMAS (Am. J. Ob. Gyn. 199.: 473e, 2008)
Many produce estrogens; a few produce androgens. They almost never act malignant unless there are a lot of mitoses.
For some reason, they are prone to cause ascites and sometimes even hydrothorax ("Meig's syndrome). Nobody knows how (* possible serum factors: Am. J. Ob. Gyn. 184: 354, 2001; prefers the right side of the chest for unknown reasons
* Future pathologists: There's probably no reason to try to distinguish a thecoma (which may have been hormonally active) from a fibroma (which wasn't) on pathology. The tumor is out. True fibroma? Think of Gorlin's.
Most produce androgens; a few produce estrogens. Androgens from these tumors (or any other source) will tend to defeminize (i.e., stop the monthly cycle) and masculinize (=virilize, i.e., enlarge the clitoris, produce extra body hair, altered hairline, acne, more apocrine sweat, deep voice).
Look for Reinke crystalloids in the Leydig cells.
MISCELLANY:
"Hilus cell tumors" are composed only of Leydig cells. They produce androgen.
Steroid cell tumors (formerly "lipid cell tumors") are benign, full of yellow lipid, and usually virilize. "Pregnancy luteoma" is a massive corpus luteum.
"Gynandroblastoma" is a mix of male and female sex cord type cells.
"Gonadoblastoma" occurs in abnormal gonads ("intersex" people, "gonadal dysgenesis") -- undifferentiated gonadal tisue: J. Clin. Endo. Metab. 91: 2404, 2006. You'll see both eggs and a mix of sex-cord and stromal tumors, usually with a lot of calcifications. They are benign but may transform, usually into dysgerminoma.
|
|
|
|
|
|
|
|
|
|
{49415} hydrops fetalis
{49416} fetal death, cord around neck
|
|
EXAMINING THE PLACENTA (still good: Am. Fam. Phys. 57(5), March 1998)
Here's what to look for:
Thick / big placenta: Diabetes? Hydrops fetalis? Infection? All these should be known to you already.
Big blood clot? Suspect that there was an abruption!
A few cotyledons fibrotic? Old infarcts. A few cotyledons overly red? New infarcts. Infarcts happen and unless they are involve more than 5% of the surface (typically much more), nothing to worry about.
Pale? Is the baby anemic? Is Mom bleeding out?
Soft? Infection?
Fleshy, dark red blob? CHORANGIOMA (CHORIOANGIOMA). A benign hemangioma, of no consequence unless it is huge, in which case it acts as a shunt, consumes the baby's platelets, and can cause congestive heart failure.
An accessory lobe, separated from the main placenta by vasculature, is called a SUCCENTURIATE LOBE and the membranes are often attached. If by misfortune this overlies the cervix, it's likely there'll be bleeding. A BILOBATE placenta, with equal-sized lobes, carries the same risk.
CIRCUMVALLATE PLACENTA: The basal plate (mom's side) is quite a bit bigger than the chorionic plate (baby's side); this will appear as a ring around the edge on the fetal surface. This can cause various problems as you'd expect, since the baby's wrapped up inside. A CIRCUMMARGINATE PLACENTA is a forme fruste that's not so worrisome.
AMNION NODOSUM is vernix caseosa embedded in the amnion. Usually there's oligohydramnios. It should not be confused (though some do) with the harmless squamous metaplasia you can see here especially near the insertion of the cord.
Any amniotic bands?
Green? Meconium or pus, less likely biliverdin from an older bleed.
Peculiar odor: Infection. Listeria may smell sweet, others will be malodorous.
Cord:
VELAMENTOUS INSERTION is a cord attached to the membrane but away from the placenta. It occurs in maybe 1% of placentas and supposedly places the child at greater risk.
SPONTANEOUS ABORTION
About half of miscarriages supposedly have a chromosomal abnormality. You'll go crazy trying to sort out what's known (and what's not) about the other causes, which include "failure to implant" (nobody knows how common this is), disappearance of the corpus luteum "because of other endocrine disease", "incompetent cervix", low folic acid/B6 (i.e., poor diet -- does this run with some other lifestyle-related risk factor? JAMA 288: 1867, 2002; Ob. Gyn. 100: 107, 2002), and of course antiphospholipid antibody and (especially later in the course of the pregnancy) congenitally hypercoagulable blood (NEJM 343: 1015, 2000; Ann. Int. Med. 130: 736, 1999; Factor V-Leiden is now infamous and generally the thrombophilias are well-established causes of loss of pregnancies -- "prothrombin G20210A" is evidently an exception Ob. Gyn. 115: 14, 2010). Contrary to older ideas, nowadays assisted reproductive technology probably isn't a risk for loss later in pregnancy (Ob. Gyn. 114: 818, 2009).
Amniotic band syndrome probably results from the healing of tiny leaks in the amnion; it is a common cause of miscarriage and can result in damage to body parts in a baby that makes it to term. If the amniotic sac ruptures early in pregnancy (perhaps related to amniotic band syndrome), an astute pathologist can spot vernix (desquamated cells from the baby) in granulomas in the lost tissue.
BLIGHTED OVUM / ANEMBRYONIC PREGNANCY features a good placenta and membranes but no baby (due to a known or unknown genetic defect -- some of these are triploid and this fades into moles). It is common and now easily recognized on ultrasound; often this is a sad surprise for a woman who think she has a normal pregnancy. The pathologist will eventually see the villi; unlike hydatidiform mole, there's atrophy rather than proliferation of trophoblast, and the edema of the villi isn't impressive.
Previous elective abortion (either surgical or by the increasingly-popular methods involving taking medication) do not seem to place a woman at risk for future miscarriage or ectopic pregnancy (NEJM 357: 648, 2007).
Today there is some interest in bacterial vaginosis and chlamydia as causes of loss of the unborn child before viability (Am. J. Ob. Gyn. 183: 431, 2000; others).
After a miscarriage, curettage of the endometrium yields necrotic tissue, often intensely inflamed with neutrophils. There will of course always be decidua, and often villi if they have not been passed.
* Lancet 371: 290, 2008 reports that 68,000 women die yearly from unsafe elective abortions in countries where the procedure is illegal. Obviously, this is an estimate, and I don't understand how it was reached.
PREMATURE DELIVERY
The most important single cause of premature delivery is premature rupture of the membranes. You'll learn a great deal about this on OB. Old lab tests (ferning, nitrazine for pH, fat stain after 32 weeks for fetal sebum, injection of dye into the sac itself) are all fraught with problems. Watch for IGFBP-1 and PAMG-1 (placental alpha-macroglobulin 1 / "Amni-Sure") as point-of-care tests for the presence of amnionic fluid.
No one really knows how often problems with the cord cause the child's death, but it must be fairly common.
Often the dead child remains in the amniotic fluid for days or weeks, and pathologists can estimate the time since death of these "macerated" babies. (The unborn child is in a sterile environment and thus autolyzes rather than putrefies.) A "papyraceus" fetus is a twin who died and whose body was flattened by the other child's.
In the industrial world, rates of stillbirth dropped dramatically during the 1940's -- no one knows why, but your author suspects it has to do with the ability to treat urinary tract infections. Rates of stillbirth have afterwards remained steady -- no one knows why, but your lecturer believes it has to do with obesity and lack of exercise and women smoking balancing what we can hope is somewhat improving prenatal care. See Lancet 377: 1703, 2011.
ECTOPIC PREGNANCY (Am. Fam. Phys. 72: 1707, 2005; JAMA 309: 1722, 2013)
The usual location is the oviduct, though ovary, peritoneum, and uterine cornua are other known sites. Rarely an intraperitoneal pregnancy goes to term.
The best-known cause is old pelvic inflammatory disease (classically gonorrhea; chlamydia is also very much a culprit J. Inf. Dis. 207: 30, 2013), less often scarring from endometriosis. But about half of cases in the US happen "for no reason." In countries where there is much more gonorrhea, there are many more ectopic pregnancies.
No matter where the pregnancy is, the local cells decidualize and the child develops for a while. In a tubal pregnancy, disaster strikes at about 6 weeks after the missed period (about 8 weeks after conception). One of the following happens:
Nowadays these are usually found on a transvaginal ultrasound. Treatment is surgical. Or if an ectopic pregnancy is known to be present but has not ruptured, methotrexate can terminate it easily and safely.
|
|
![]() 9 week fetus
9 week fetus
Ectopic pregnancy
Wikimedia Commons
PROBLEMS IN LATE PREGNANCY
Many of the problems that develop toward the end are caused by problems with the umbilical cord. Of course, if the cord is compressed enough to occlude the veins, the child is in grave danger. This includes slip knots, cord around neck, or cord being compressed by the child's head against the cervix.
Infections can pass through a ruptured membrane
and produce
inflammation of the chorion, amnion (chorioamnionitis) and cord (funisitis).
Common bacteria (a pathologist can spot fusobaterium using a silver stain)
can infect the placenta (villitis, chorioamnionitis), as can syphilis![]() ,
toxoplasmosis
,
toxoplasmosis![]() ,
and TB
,
and TB![]() . If you see granulomas, think of listeria.
A chlamydia infection is likely to produce red eyes in the newborn.
The one established fungal culprit is candida (look for classic "thrush" on the
umbilical cord). In malaria
zones, involvement of placenta often permanently damages the baby (Hum. Path. 32: 1022, 2001).
Thankfully there's
not much brucellosis in the US any more.
. If you see granulomas, think of listeria.
A chlamydia infection is likely to produce red eyes in the newborn.
The one established fungal culprit is candida (look for classic "thrush" on the
umbilical cord). In malaria
zones, involvement of placenta often permanently damages the baby (Hum. Path. 32: 1022, 2001).
Thankfully there's
not much brucellosis in the US any more.
* If you look really hard, in 10% of placenta you can find Mom's T-cells in Baby's villi, with patchy chronic inflammation which we may suppose is due to immunity against Dad's antigens. Just how often this is a real problem is unknown.
* And if you look really hard, you can find plasma cells and/or real-looking chronic inflammation in 3% or so of term deciduas ("chronic deciduitis"). What this means is unknown.
ABRUPTION OF THE PLACENTA is a huge bleed between the placenta and the wall. It is among the most dreaded obstetrical complications.
PLACENTA PREVIA occurs when the placenta covers the lower uterine segment over the cervical outlet. This can cause premature labor by affecting the placenta. As the cervix dilates, bleeding occurs.
{15876} abruption of the placenta, sectioned in situ
* The molecular biology is only now being worked out, and it's complicated, with growth factors involved in invading trophoblast transforming it from epithelium to mesenchyme (Am. J. Ob. Gyn. 204: 411, 2011).
You remember the mnemonic for the infections of the unborn child:
* Pathologists are just now starting to examine placenta changes in children with cerebral palsy, and the results are not very surprising: clots, partial abruption, inflammation, widespread infarction (Arch. Path. Lab. Med. 124: 1785, 2000).
* Fun to know: Cesarean section means "to cut". It has nothing to do with Julius Caesar or laws that he passed. Even in ancient times, it was routine to take the child by C-section when it was obvious the mother would die.
* The old rule was, "Once a cesarean, always a cesarean." In the early 1990's, politics for some reason dictated that "every women deserves a trial of vaginal delivery no matter how many cesarean sections she's had previously". This became a "cause for women's advocates" who distributed "informational literature", and then became a mandate by practice groups and third-party payers. And as any reasonable person would expect, it led to a great many catastrophic deaths (uterine rupture, placenta accreta, amniotic fluid embolization). For an account of the fiasco, see ACOG Practice Bulletin 104: 203, July 2004. Today, the practice recommendation is that as long as there's been only one cesarean section, and it was with a low-transverse incision (or maybe a lower-segment vertical incision), and resuscitation is available in case of disaster, the woman should be given a CHOICE of a trial of vaginal delivery. DON'T try vaginal delivery if there was a classical incision used for the cesarean section.
|
|
|
|
TWINS
Think about it.
One chorion, two amnions: A membrane separates the children, but it contains only an amniotic layer, not a chorionic layer. They must be monozygotic twins. Okay, there was one reported exception: NEJM 349: 154, 2003 (in vitro fertilization, donor oocytes).
Two chorions: A membrane or two separates the children, and contains both chorion and amnion. They may be monozygotic or dizygotic (fraternal) twins. Dichorionic placentas can be separate or fused.
The major hazard is a one-way channel between the twins' umbilical cords. This causes chronic twin-twin transfusion syndrome. The twin who gets the blood will be big and can die of circulatory overload. The twin who loses the blood will be small and can die of anemia. Repairing it in-utero: Am. J. Ob. Gyn. 198: e4, 2008. Today we use lasers.
An "acardius" is a very malformed fetus with no heart. It can survive if it is anastomosed to a normal twin.
TOXEMIA OF PREGNANCY (Am. Fam. Phys. 70: 2317, 2004; Lancet 376: 631, 2010)
Somewhere in the world, a women dies every three minutes from causes related to toxemia of pregnancy (Curr. Op. OB-Gyn, 14: 119, 2002). The longstanding mystery of toxemia of pregnancy is just now being clarified.
The key molecule is probably sFlt1 (now "soluble vascular endothelial growth factor receptor-1, sVEGFR-1), a tyrosine kinase that binds to VEGF and other factors. This ends up having a variety of actions on blood vessels, including inhibiting their growth and causing them to leak (J. Clin. Inv. 111: 600, 649, & 707, 2003; NEJM 350: 672, 2004; Hypertension 55: 689, 2010; animal model is now established Am. J. Ob. Gyn. 205: 266, 2011). Ordinarily, this is the "brakes" on vascular proliferation late in pregnancy. In toxemia of pregnancy, it appears too soon. There are other factors involved as well, and it will take more time before this hormonal symphony is sorted out (J. Clin. Endo. Metab. 95: 1431, 2010).
The process begins when the placenta becomes ischemic. Poor trophoblastic invasion, insufficiency of the uterine arteries, or goodness-knows-what sets it up. Once begun, a vicious cycle starts. Something (evidently sFlt1, maybe other stuff) is released by the ischemic placenta that causes endothelial swelling (raising blood pressure) and leakage (proteinuria and edema), and damage sufficient to produce DIC.
* If the toxemia has appeared relatively early in pregnancy, vessel changes and signs of ischemia are more marked (Am. J. Ob. Gyn. 210: 66, 2014).
"The usual suspects" produced by the ischemic placenta -- thromboxanes, angiotensin, endothelium, and so forth -- need not concern the classroom pathology student.
So far, we have pre-eclampsia -- which you will diagnose clinically when the blood pressure exceeds 140/90 (measure twice, not at the same time) AND there's 300 mg or more of the protein in the urine per day..
When the woman has had a seizure, it's "eclampsia" and the mother and baby are both at grave risk.
Further, lethal disease in one twin is likely to cause pre-eclampsia that can be cured by destroying the affected twin to permit safe continuation of the remaining twin's gestation to term (Am. J. Ob. Gyn. 191: 477, 2004).
* Perhaps the reason that it occurs most often in the first pregnancy is the finding (awaiting confirmation) that women who have had very little (<4 months) exposure to the father's semen are at much greater risk (Am. J. Ob. Gyn. 188: 1241, 2003). Can you think of why this makes sense? Remember that half of the placental antigens are contributed by Dad. If you are not prudish, see J. Repro. Imm. 46: 155, 2000 for a correlation between a popular practice between husband and wife and how it seems to protect from pre-eclampsia. Follow-up on "seminal priming" J. Repro. Imm. 59: 253, 2003 ("... or else as a sublingual spray.")
In other words, pre-eclampsia is considered non-preventable. However, restricting sodium, resting, and maybe prescribing antihypertensive medications can stave off eclampsia.
The morphology of eclampsia is distinctive. (We may suppose that milder versions of these changes would be seen in pre-eclampsia.)
Update on the histopathology: The clincial correlation with the pathology is so-so (Am. J. Ob. Gyn. 194: 1050, 2006).
Delivery is curative.
When there is also hemolysis, elevated liver enzymes, and low platelet count (findings that typically run together), we make the additional diagnosis of HELLP (Hemolysis, Elevated Liver enzymes, Low Platelets) SYNDROME. I've predicted that the placenta produces some toxic factor that remains to be discovered; there is now a report that it is CD95, the fas ligand (Gastroent. 126: 849, 2004) and/or endothelin-1 (J. Clin. Endo. Metab. 90: 4205, 2005). There are more players as well, and the process is obviously a complex mix of problems (Am. J. Ob. Gyn. 194: 317, 2006). As with acute fatty liver of pregnancy, an autosomal-recessive locus has been found (J. Clin. Inv. 122: 4003, 2012).
HYDATIDIFORM MOLE (Am. J. Ob. Gyn. 203: 531, 2010)
About one pregnancy in 1000 in the US is a mole. It's much more common in China and Southeast Asia.
A hydatidiform mole looks like a mass of grapes, as each villus swells up. The pathologist will see villi with very poor or absent blood vessels (i.e., mostly just myxoid stuff; after all, there is no fetal heart to perfuse the chorionic vessels) and a lot of edema. Hippocrates called it "dropsy of the womb".
"Partial" moles (twice as common as classic moles) have unevenly swollen villi, trophoblastic proliferation is patchy and mild, and they are triploid -- 69,XXY or 69,XXX. The extra set can come from either parent. There's also at least one autosomal recessive locus (NLRP7/NALP7) that will turn what should have been a baby with 23 chromosomes from each parent into a complete mole (Arch. Path. Lab. Med. 136: 646, 2012).
* Future pathologists only: In a miscarriage due to hydrops fetalis (i.e., marked edema of the child), the specimen will resemble a hydatidiform mole without any atypia (distinguishing it from a complete mole) and disomy or near-disomy and positive p57 staining (distinguishing it from a partial mole; update Am. J. Surg. Path. 36: 1747, 2012).
The two lesions can't always be distinguished histologically. A triploid/partial mole is much less likely than a diploid mole to go on gestational trophoblastic disease (Cancer 100: 1411, 2004). Update on the clinical features: BJOG 114: 1273, 2007.
* You can be a good doctor without knowing the karyotypes of hydatidiform moles, but it's a triumph of science and a favorite trivia question. Future truly hardcore pathologists: You can tell a partial mole from a complete mole because the former stains with a p57kip2 that is only expressed from the maternal chromosomes (Am. J. Surg. Path. 25: 1225, 2001).
Usually the uterus is larger than it should be, and bleeding and loss occurs in the fifth month. If the serum hCG levels have been monitored, they are higher than normal.
If there is a normal twin, and Mother wishes to take the pregnancy to term, super-specialist consultation is indicated and has about a 40% of producing a healthy baby.
Once delivered, the clinicians will check for persistent hCG in the serum. This happens after about 20% of complete moles and around 4% of partial moles. If elevated, the diagnosis of PERSISTENT GESTATIONAL TROPHOBLASTIC DISEASE will be made and the tissue removed by curettage.
If it is a complete mole, around 3-5% of women with persistent gestational trophoblastic disease will develop invasive mole or choriocarcinoma ("daddy's bad girl"). Partial moles almost never do this.
Grossly, the tumor is mushy and ultra-bloody (since trophoblast by its nature invades blood vessels). The tumor has always disseminated widely by the time it is diagnosed.
Microscopically, there will be no villi. The pathologist will see cytotrophoblast and syncytiotrophoblast, usually in alternating layers.
Formerly, this was uniformly lethal. Today, the large majority are cured with chemotherapy.
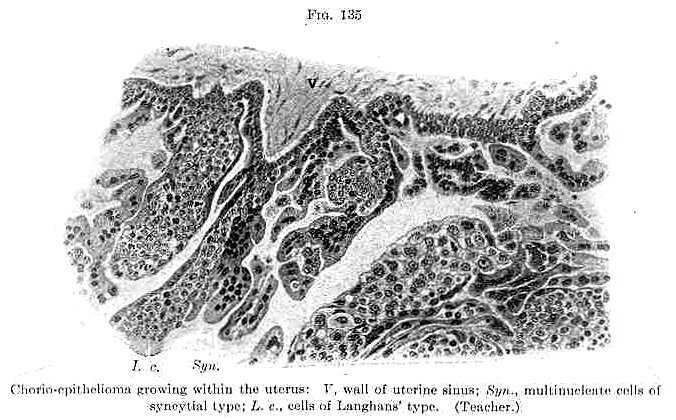 Choriocarcinoma
Choriocarcinoma
Classic drawing
Adami & McCrae, 1914
![]() Choriocarcinoma
Choriocarcinoma
Tom Demark's Site
* There are several other lesions involving gestational trophoblast. Leave their diagnosis to us. "Exaggerated placental site" is a non-problem. "Syncytial endometritis" / "placental site nodule" calls for serial hCG measurements but usually causes no trouble. "Placental site trophoblastic tumor" is a cancer composed of variant trophoblastic cells and produces human placental lactogen (and maybe don't produce hCG). It usually follows a normal birth, lacks the extreme anaplasia of a real choriocarcinoma, and produces a distinctive glomerular lesion with fibrin and IgM in the loops (Ob. Gyn. 114: 465, 2009). There are a few other obscure gestational cancers. Some choriocarcinomas take the forms of other familiar carcinomas, especially squamous.
![]() {47859} pregnant
{47859} pregnant
* Acupuncture and other "alternative" medicines (with the exception of black cohosh and phytoestrogens) completely fail for relief of menopausal syndromes (Ann. Int. Med. 137: 805, 2002). "Vitex" (Chasteberry, named for its known-for-centuries effects on sex hormones that are obvious but still not understood) passed a small Louisiana study glowingly as a treatment for PMS; women also say it works for cyclic mastalgia.
When politicians get involved, the real losers are usually ordinary, decent folk. As physicians, you are called to bring reason and science into public discussions. Again, the following "women's health issues" unit is non-testable.
ESTROGEN REPLACEMENT: In summer 2002, the first big prospective randomized study of the health effects of estrogen-progesterone replacement was stopped early because the treatment group was having more cardiovascular problems and breast cancer than the controls. Especially the cardiovascular effects were opposite to the "conventional wisdom" that replacement is beneficial. If the conventional wisdom is indeed incorrect, perhaps it reflects that women who go to the doctor more often are both healthier and more likely to receive hormone replacement. Gee whiz. Watch this business. Another study found that replacement increases the risk for venous thrombosis and gallstones (JAMA 288: 99, 2002), without much beneficial effect on fracture risk. The fact that there wasn't an impressive impact on fractures obviously results from the study covering only a few years, which was stupid, and the slightly higher mortality rate in the treated group doesn't look statistically significant. The media parlayed this into estrogens causing tremendous cardiovascular risk, and there will be trouble for the next several years over this.
THE BENDECTIN FIASCO: The United States pays the price for its tort system and ignorance of science.
In 1983, the best drug for severe nausea and vomiting of pregnancy (doxylamine, marketed with pyridoxine as "Bendectin" by Merrell-Dow) was withdrawn because of lawsuits alleging the medicine had caused babies to be born deformed.
The hoopla followed an exposé in The National Enquirer (1979). The principal researcher alleging that Bendectin was a teratogen was denounced by his own co-workers as a blatant fraud (JAMA 263: 1468, 1990). Other animal studies supposedly demonstrating teratogenicity found similar effects for sugar and tap water, but could not show a teratogenic effect for thalidomide (JAMA 264: 569, 1990). The NIH epidemiology found no link whatever (Teratology 40: 151, 1989). I found a single recent abstract (89300349) alleging a link, and it is an sorry effort from the former Soviet Block, where there has been no real biology since nature-mystic Thaddeus Lysenko oversaw Stalin's extermination of his country's honest biologists. However, as late as mid-1994, a jury awarded $19 million to a kid whose mother (Ms. Daubert) took Bendectin; the kid's only problem was common clubfoot. Last case thrown out: Science 267: 167, 1995.
Almost all the other lawsuits were unsuccessful, but had placed a tremendous burden on the corporation. The whole business went to the Supreme Count, which in 1993, in a solid, landmark decision ("Daubert vs. Merrell Dow"), required judges to bar junk science from their courtrooms (JAMA 270: 423 & 2964, 1993; Science 261: 22, 1993, thanks Mr. Justice Scalia). Good luck. Nowadays, nobody is going to market a drug for use by pregnant women, or a vaccine, or anything else that invites silly lawsuits. As usual, it is the people who are really sick who suffer. Review of the whole business: NEJM 370: 1081, 2014.
Of course, today doxylamine and pyridoxine are offered as a combination to treat morning sickness.
THE PAP SMEAR FIASCO: The United States pays the price for its tort system and ignorance of the limits of screening.
The pap smear for cervical cancer was designed as an inexpensive screening test. The key was "inexpensive". The consensus among pathologists is that a 10% false-negative rate is quite acceptable, and if it's that low, probably even good practice. (College of American Pathologists, cited in Path Yearbook 1994 p. 42). The idea was that the test should be repeated frequently, in case the technician misses a few cancer cells on one slide.
Unfortunately, the lawyers and militants got into the act in the mid-1980's. ("Murderers" missed a few cancer cells on pap smears; this is likely to be fatal only if the women aren't screened as often as they should be.) The price of a "pap smear" rose from $5 to over $50 because of all the regulations; I haven't seen anything to suggest that quality is better, and "to save money", lots of gynecologists switched to a one-slide specimen, which means less sensitivity but much better cover-your-butt. The result, of course, was that the test became unavailable to the underclass women who are at greatest risk, and the rate of invasive cancer of the cervix has increased. See Med. Care. 30: 1067, 1992; Acta Cytol. 36: 461, 1992.
FEMALE GENITAL MUTILATION: ("female circumcision"); Women in the world's poorest nations suffer, while the rich nations ignored a horrible problem for ideological reasons.
The custom is most common in Africa, where some people believe it ensures a woman's chastity and, after she is married, her fidelity by reducing sexual pleasure.
-- Br. Med. J. 313: 1103, 1996.
Until 1992-4, the abominable practice of female circumcision was a taboo subject, thanks to the politics of the era. ("You cannot criticize these people's culture.") In 1994, the medical literature (until then, strangely silent) suddenly was filled with physicians saying the obvious: FEMALE CIRCUMCISION IS A CRIME AGAINST HUMANKIND.
What is female circumcision? It's a "cultural practice" to which around 100,000,000 living human females have been subjected, mostly in Africa north of the equator. For example, almost every human female in Somalia is circumcised. It involves the surgical amputation of the clitoris, sometimes with the surrounding tissue, part or all of the labia majora, and/or the labia minora. Sometimes the introitus is sewn shut with needle and string, and the new husband cuts the string when he buys the wife. It's usually performed on children, often with no anesthetic. What's the basis for this "cherished traditional cultural practice"? The intent, of course, is to make the girl less interested in sex, and less able to do it, so that she will be a virgin when she is ready to marry and will therefore get more money for her parents.
Complications include huge dermoid cysts arising in the scar, loss of sexual pleasure, inability to menstruate, inability to have intercourse, pelvic and back pain, chronic pelvic infections leading to stones and hydroureters, stitch abscesses, traumatic neuromas, reopening of the incisions, pain on intercourse, vesicovaginal fistulas (dribble continuously), and catastrophic problems with delivery of children. Every one of these is common. Unlike male circumcision, there are no health benefits whatsoever. Opposition to female circumcision comes from mainstream Islam (Saudi Medical Journal 21: 921, 2000, thanks) and Christianity, and even the WHO, which in 1992 (after knowing about the problem since its founding, of course) finally condemned it officially (Eur. J. Ob. Gyn. 45: 153, 1992). Here's a reading list on female circumcision, including a few pieces by Leftists who ask, with a straight face, whether concern for health can ever override "multicultural sensitivity":
Plastic and laser surgeons are able to help these women: Am. J. Ob. Gyn. 187: 1550, 2002; update Lancet 380: 134, 2012 (a year after surgery, around half of the women find intercourse pleasurable instead of solely painful.)
More changing times: Only during the mid-1990's did it become politically acceptable in the USA to talk about the endemic of violence against women in sub-Saharan Africa. The problem was and is unbelievable: JAMA 279: 625, 1998; Lancet 371: 15, 2008 (rape as a weapon to demoralize civilian populations in collapsed society of the former Belgian Congo); Lancet 373: 1966, 2009 (one girl in three in Swaziland suffers sexual violence before age 18, often by family, friends-of-family, or in school.) Ninety-one Sudanese women who had been rendered totally fecal-incontinent from sexual violence: Lancet 354: 2051, 1999. "What are the human rights of a teenager who is the third wife or a man the age of her grandfather who will not allow her to use contraception even though her last confinement nearly killed her?" (Br. Med. J. 321: 570, 2000). In some communities in Pakistan, it is considered "honorable" to kill your daughter if she wants to make her own choice about who she marries (BMJ 338: b1221, 2009); there are dozens of such killings each year. It seems to me that "cultural practices" or no, something is wrong if it interferes with people's health. The Taliban's oppression of women, and the resulting impact on women's health, was frightful: JAMA 280: 449, 1998. The extent of Saddam's organized violence against women, especially against Shi'a women between 1991 and 1993, is astonishing (JAMA 291: 1471, 2004).
ATTENTION TO WOMEN'S PROBLEMS: Right or wrong, it's human for each individual to interact differently with males and females, even when pursuing gender-neutral activities, and in this regard, every human being's behavior is different. Where things go wrong is when fairness is compromised, as in the old days, when medical schools wouldn't take women "because they'll just get pregnant and then never practice." That really happened, and happened frequently. Things are better since the 1950's ended, at least in this regard. Thankfully it's now possible to punish those who really commit sexual harassment, which has historically been the bane of a professional woman's existence, in the health-care setting and otherwise. But there's still a tendency by physicians to thoughtlessly ignore health problems specific to women. In one chart review (at an M.D. institution, mind-you), housestaff (male and female) doing history-and-physicals almost never asked about pap smears, mammograms, or breast self-exam, and were only half as likely to do breast exams (35%) as to do a rectal (70%). When I was a med student, I was, to my knowledge, the only one who discussed breast self-exam with every adult female patient. See Academic Medicine 68: 698, 1994. There's plenty of evidence now that women get under-treated, or at least get less treatment for the same things, as do men. See, for example, Am. J. Psych. 150: 1309, 1994 (on being human, as well as disparities in care), JAMA 268: 1872, 1994 (women alcoholics get less care than men), Arch. Int. Med. 152: 972, 1994 (women with myocardial infarcts get treated less aggressively; the latter effect might be due to women being better protoplasm and less sick than men: NEJM 330: 1101, 1994). Hip arthroplasty: NEJM 342: 1016, 2000. Reperfusion in heart attack: NEJM 342: 1094, 2000. Docs: Unless you want Uncle Sam to get involved, you need to do something about this yourselves. And this should come as no surprise: In India, where most families supposedly want sons rather than daughters, three girls die of diarrhea for every boy (Br. Med. J. 327: 126, 2003). South India has by far the highest known suicide rate of anyplace in the world; most often, it is a young woman who commits suicide rather than be forced to marry a man she hates (Lancet 363: 1117, 2004). Women in many traditional societies commit suicide to avoid forced marriage or escape domestic violence (NEJM 358: 2201, 2008). Well over half of all wives in Yemen are beaten or worse (Am. J. For. Med. Path. 33: 163, 2012) -- your lecturer's personal conversations have led us to believe that men from this kind of culture "hate America" because we treat women decently and want others to do so as well. Call me something bad if you want. Click here for the Archbishop of Canterbury's remarks after England passed an act protecting its women from forced marriage. This was quoted out of context by outraged militants of various kinds, resulting in a world news story.
IN-VITRO FERTILIZATION: Some people say it's your inalienable right to have Uncle Sam pay for it, while for others, it's anathema on religious-ideological grounds. Averages: To get one born baby when all the factors are favorable, somebody will pay $50,000 if it works the first try; when there's male-factor infertility and five previous failures, the cost is $800,000 per baby (NEJM 331: 239, 1994). I bet third parties (Uncle Sam, managed care) won't pay for this.
FETAL MONITORING is fancy-tech, and since it's available, the savvy physician has to use it to cover his butt. However, the benefits to the human race are by no means apparent, and people are finally getting up the courage to say so (Can Med. Assoc. J. 148: 1737, 1994; J. Fla. Med. Assoc. 78: 303, 1994). Even the American College of Obstetricians and Gynecologists has come out with a statement that listening occasionally with the stethoscope is every bit as good as hooking up a monitor (Ob. Gyn. 76: 1130, 1994; this has held up). There are more muddy-the-waters technologies on the horizon; there's no reason yet to think they'll do much to help patients, though they'll surely increase health-care expenditures and incomes (Curr. Op. Ob. Gyn. 5: 647, 1994; Br. J. Ob. Gyn. 100: 733, 1994). One fancy intervention ("home fetal monitoring") didn't seem to do much that simply explaining things to the patient didn't (Am. J. Ob. Gyn. 164: 756, 1994). This trend has continued to the present; in the "managed care" era, the decisions of obstetrician-gynecologists about which technologies to use are a curious subject (Am. J. Ob. Gyn. 188: 162, 2003); a Canadian group points out the obvious fact that "defensive medicine" can itself generate income for physicians (Soc. Sci. Med. 51: 523, 2000), etc., etc. Especially welcome is the loss of the fetal scalp blood monitor as a standard of care.
Androgens for female sexual dysfunction / low libido: Mayo Clin. Proc. 79(4S): S-19, 2004. No joke -- when one partner loses interest in sex, the effect on a marriage is often devastating.

Goya's sketch of women resisting
For more on the vile crime of RAPE, check the current literature. There are around 20,000 convictions per year in the USA for adult rape, and 23,000 for child sexual abuse. Examining and treating the woman who has been raped: NEJM 332: 234, 1995; Ped. Clin. N.A. 46: 809, 1999. Dudes: Forcing yourself on an unwilling woman is the most un-masculine thing you can do. Most rape is committed by an acquaintance, and (despite what's below) I suspect most rapes go unreported, which is bad. "Roofies" is flunitrazepam ("Rohypnol"), which when added to her drink makes rape easy (review South. Med. J. 93: 558, 2000). One bizarre article even cites industry-specific rates for being raped by a co-worker (Am. J. Pub. Health 84: 640, 1994). Under the common law, a husband may lawfully penetrate his wife without her consent; this is changing. The serial rapist generally starts shortly after puberty, as a stupid-hurtful way of expressing anger. The first victim is usually an acquaintance. In most jurisdictions, rape means putting any part of his penis into any part of her body without her consent. In others, it may include putting something else into her vagina or anus without her consent. (Contrary to what you may have read in the magazine article, unwanted touch through clothing is not rape.) He doesn't have to have an erection, he doesn't have to ejaculate, it doesn't have to be her vagina, it doesn't matter if she's known to be easy, or if she consented last night, or if she happily took off her clothes and got in bed with him, or was petting for a long time, or if she just teased him, or said she would and then changed her mind, etc., etc. A man can get raped, too. A mentally-retarded or very crazy person cannot lawfully consent, no matter what her age. Dudes: if she changes her mind later, and says you raped her, it's her word against yours. Nowadays, the law and public opinion are stacked against you in this (and many other situations, too) simply because you are a man. For example, a judge isn't even allowed to remind a jury that it's easy to bring a false accusation or rape, and hard to defend against it, and the defense may not even be allowed to present evidence that a particular woman had already made a previous false allegation "because it might inflame the jury" (Arkansas Supreme Court, Ralph Taylor). "Rape shield laws" forbidding any discussion of the accuser's previous sexual history have been interpreted to include the accuser's currently facing criminal charges for having consensual sex with minors (Charles Steadman, 1993). In some juristictions, the law specifically allows that a man can be convicted of rape solely on the uncorroborated testimony of an accuser, without any physical evidence whatsoever. This results from litigation from the 1970's prompted by militants, including the author of "Against our Will: Men, Women, and Rape", whose mentality is illustrated by her statement that rape is "nothing more or less than a conscious process of intimidation by which all men keep all women in a state of fear." Be careful, dudes, especially around people you don't know aren't "fantasy-prone", mentally-ill, or malicious or worse. However, until 1994, the subject of "factitious rape", i.e., a woman making a false accusation, was a forbidden subject in the medical literature for political reasons, and patently false ideology ("No woman would lie about something so personal"; "The FBI has proof that only a few percent of claims are false", etc., etc.) dominated discussion. That false claims get made, and that they are very difficult to defend against, has been documented for over 3500 years -- remember Potiphar's wife, Phaedra and other tales from the classics. A major article by the US Air Force Office of Special Investigations that got no attention at the time appeared in Forensic Science Digest 11(4): 64, December 1985; of accusations of rape brought in the Air Force, a panel of three reviewers unanimously agreed 60% were false, with many of the women recanting before or after failing a polygraph. The landmark article appeared in Arch. Sex. Behav. 23: 81, 1994. Now that we have DNA testing, it's become clear, in retrospect, that plenty of men serving prison time for a particular rape didn't do it (KC Star March 13, 1993 was the first in what has now become a frequent feature of new stores.) The now-classic 1996 article from the US Department of Justice "Convicted by Juries, Exonerated by Science" cited a statistic of 25% for cases in which DNA specifically excludes the accused; this does not include those for which results are indeterminate, and of course it does not exclude the possibility that the sex was consensusal (remember the defense in the Kobe Bryant case). By 2008, there have been over 200 convictions overturned -- all men were serving long prison terms. This is in keeping with my own experience doing exams, which range from godawful cases of genuine rape to women trying to get out of a non-rape abusive situation to malicious women simply trying to get a particular man in trouble. The latter works. My reading of law articles indicates there are perhaps 33,000 false accusations of rape per year in the US, primarily against African-American men. "Rape counsellors": Before you tell her absolutely to... please be sure that.... Your lecturer doesn't take anybody's word on anything any more, in the absence of physical evidence. He also considers himself a macho-man, and is glad that the same science that now protects a man against a false claim of rape also brings real perpetrators to swift justice. For "Factitious rape", see South. Med. J. 87: 736, 1994; Arch. Sex. Behav. 23: 81, 1994 (the latter found 41% of police rape accusations to be false; my informal series in 1982-3 was at least this high). Self-inflicted wounds by a women claiming to be raped: Am. J. Forens. Med. Path. 20: 374, 1999; Med. Sci. Law. 38: 202, 1998. Wood's lamp is notoriously nonsensitive and nonspecific in looking for semen: Pediatrics 104: 1342, 1999. Examining the clothing can support a claim (saving the woman a terrible ordeal) or refute a claim (saving the man a terrible ordeal) -- the authors of this paper talk about the "sensitive" politics: J. Forens. Sci. 45: 568, 2000. The false memories syndrome has produced women who accuse both family and physicians of terrible crimes -- for a case of a woman with uterine agenesis who "remembered" incest, a resulting pregnancy, and a resulting criminal abortion by a particular physician: J. Ped. Adol. Gyn. 11: 181, 1998. (A few years before, it would have been extremely difficult to defend against this accusation.) As I mentioned, you will find nothing whatsoever on this very important subject in the English-language medical literature before 1994. Today, before love happenes, he should text her, "I want you" and she should text back "I want you." How romantic -- and the perfect defense should there be a misunderstanding.
Current dogma in "child sexual abuse" circles is that a normal physical exam is consistent with any manner of horrid abuse, including recent full penetration of a baby girl by an adult male's erect penis. This strange idea is based on misrepresenting the actual data from an article in Pediatrics 94: 310, 1994, rebutted Pediatrics 97: 148, 1996. The best study so far on healing of the hymen (Pediatrics 119: e1094, 2007) does document that it heals well, like the buccal mucosa, often without marks. Even an 8-month-old girl healed with only neovascularity at the site of previous transection. Of course, this makes it much more difficult to defend against a coached accusation. A problem that I have with this paper, which will be of great importance in sex-abuse trials in the years to come, is a strange selectivity in discussion of the data. Despite all the talk about how well the hymen heals, and how even the worst trauma can heal without a trace, a look at the data shows that of prepubertal girls sustaining transection/laceration (i.e., what you might expect after full penetration -- and 16 of 39 children sustained these severe injuries), the vast majority did NOT heal either smoothly, continuously, or "delicately". The medical profession needs to do something about this, now, despite the political climate.
The term "commercial sex worker", the 1990's politically-correct term for "prostitute", was popularized by the Thai government. Free enterprise brought about "Thailand's economic miracle", which was based largely on sex tourism (Lancet 352: 246, 1998). Girls became CSW's to escape grinding poverty, and the majority paid with their lives when they contracted HIV. This seems to me to be a very great evil, and not something we want to honor and dignify by changing our terminology. Thankfully, with the decline in "political correctness", the term is now changing to "trafficked women", re-emphasizing that these women lose their freedom, their dignity, and their health, especially when they are brought from the poor nations to the rich nations as sex slaves (Lancet 363: 564, 565, & 566, 2004).
In the late 1990's, some countries took my advice and made estrogen-based emergency contraception ("morning-after pill") readily available without a special prescription. It was safe and was not abused. NEJM 339: 1, 1998. The progestin-only "Plan B" pill became legal with a prescripton in the US in 1999; the requirement for a prescription ended for women over 18 in 2006. A pharmacist can Rx it for a 17-year-old; a younger girl needs to see herdoctor. Maybe this is the right approach. For a time, the big flap was over a pharmacist's right not to full a prescription for the morning-after pill for his/her own religious reasons. Some pharmacies also refused to dispense out fear of being targeted by militants. Things seem to have settled down in the US secular health care system. For two decades, whether or not a _____ hospital can/should/must provide emergency contraception for rape victims has been an "issue" (Am. J. Public Health 91: 169, 2001); even Chile made emergency contraception available for rape victims in 2004 (Lancet 363: 1707, 2004) amidst massive hoopla, anti-contraception street demonstrations, refusals of local administrators to cooperate, and the _____ leadership comparing it to genocide under Hitler and Stalin. Mifepristone (formerly RU486) as a safe, effective morning-after pill without side effects: Lancet 353: 697, 1999. For over a decade, right-wing activists made tremendous political capital off keeping this unavailable. It was legalized in the last days of the Clinton administration. Curiously, we hear nothing from the militants about banning methotrexate, which is also a reliable and convenient way of ending an unwanted pregnancy. By contrast, 97% of families in sub-Saharan Africa cannot afford even a condom without a government subsidy (Lancet 369: 715, 2007). The most reliable emergency contraception is perhaps the insertion of a copper intrauterine device (NEJM 372: 1342, 2015).
* SLICE OF LIFE REVIEW
{08914} cervix, normal
{09755} cervicovaginal cytology, normal
{10271} cervix, normal
{10274} cervix, normal
{11764} uterus, normal
{11765} cervix, normal
{11766} cervix, normal
{11768} cervix, normal
{11769} breast, normal
{14949} ovary, monkey
{14950} ovary, monkey
{14965} ovary monkey (cortex), normal
{14965} ovary monkey (cortex), normal
{14966} ovary monkey (cortex), normal
{14966} ovary monkey (cortex), normal
{14967} ovary, cortex
{14968} ovary, cortex
{14969} primary follicle, normal
{14969} primary follicle, normal
{14970} primary follicle, normal
{14970} primary follicle, normal
{14971} secondary follicle, normal
{14971} secondary follicle, normal
{14972} secondary follicle, normal
{14972} secondary follicle, normal
{14973} atretic follicle, normal
{14973} atretic follicle, normal
{14974} atretic follicle, normal
{14974} atretic follicle, normal
{14975} corpus hemorrhagicum, normal
{14975} corpus hemorrhagicum, normal
{14976} corpus hemorrhagicum, normal
{14976} corpus hemorrhagicum, normal
{14977} corpus luteum, pig
{14978} corpus luteum, pig
{14979} atretic follicle, with loose pieces of granulosa
{14980} corona radiata, ovary
{14981} oviduct, normal
{14981} oviduct, normal
{14982} oviduct, normal with cilia
{14982} oviduct, normal with cilia
{14983} oviduct (uterine portion)
{14984} oviduct (uterine portion), arrow indicates oviduct
{14985} endometrium secretory, normal
{14985} endometrium secretory, normal
{14986} endometrium secretory, normal
{14986} endometrium secretory, normal
{14987} endometrium secretory (glycogen stain)
{14988} endometrium secretory (glycogen stain) glycogen stain
{14989} vagina, normal
{14989} vagina, normal
{14990} vagina, pap smear
{14991} vagina, pap smear
{15091} vagina, normal
{15091} vagina, normal
{15098} uterus, normal
{15098} uterus, normal
{15099} uterus, normal
{15099} uterus, normal
{15779} female genital organs unfixed, normal
{15780} vagina, normal
{15782} ovary and fallopian tube, normal
{15783} ovary and fallopian tube, normal
{15784} ovary, normal
{15785} ovary, normal
{15786} fallopian tube, normal
{15787} uterus, normal
{15788} uterus, normal
{15789} uterus, normal
{15790} uterus, normal
{15866} placenta, normal
{17495} uterus, normal
{17496} myometrium, normal
{20662} ovary, normal
{20662} ovary, normal
{20663} ovary, normal
{20663} ovary, normal
{20664} ovary, primordial oocyte
{20665} ovary, primordial oocyte
{20666} corpus albicans, ovary
{20667} primary oocyte, ovary
{20668} secondary follicle, ovary
{20669} corpus albicans, ovary
{20670} secondary follicle, ovary
{20671} ovary, blood vessels
{20672} corpus luteum, ovary
{20673} corpus luteum, invading vessels
{20674} granulosa layers, ovary
{20675} oviduct, ampulla
{20676} oviduct, ampulla
{20677} oviduct, ampulla
{20678} oviduct, isthmus
{20679} oviduct, isthmus
{20680} oviduct, isthmus
{20681} uterus, secretory endometrium
{20682} uterus, myometrium
{20683} uterus, glandular epithelium
{20684} uterus, glandular epithelium
{20685} uterus, resting endometrium
{20687} cervix, normal
{20687} cervix, normal
{20689} vagina, stratified squamous epithelium
{20788} endometrium
{20788} endometrium
{20789} endometrium
{20790} uterus, glandular epithelium
{20791} uterus, glandular epithelium
{20952} ovary
{20953} ovary, primary oocyte
{20954} ovary, primary oocyte
{20955} ovary, primordial follicle
{20956} ovary, secondary follicle
{20957} ovary, cumulus oophorus
{20958} ovary, atretic follicle
{20959} ovary, granulosa cells
{20960} ovary, corpus luteum
{20961} oviduct, ampulla
{20962} oviduct, peg cells
{20963} oviduct, isthmus
{20964} uterus, secretory
{20965} uterus, resting
{20966} cervix, squamocolumnar junction
{20967} vagina
{24446} fallopian tube, normal
{24666} placenta, normal
{25778} side-by-side arrangement, normal endocervical cells
{25788} honeycomb arrangement, endocervical cells - normal presentation
{25824} ciliated cells, endocervical cells (normal)
{25873} stratified squamous epithelium, normal cervix
{25875} superficial & intermediate squamous cells; normal pap
{25878} transformation zone, normal cervix
{25879} squamous & endocervical cells, pap smear - normal
{25888} endometrial cells - normal
{25891} endometrial cells - normal, stromal cells
{25893} endometrial cells - normal, stromal cells
{27128} ectocervix, normal glycogenated epithelium
{29291} endometrial cells, normal
{29294} endometrial cells, normal
{39421} trophoblast, normal
{39422} placenta, normal
{39423} trophoblast, normal
BIBLIOGRAPHY / FURTHER READING
I urge anyone interested in learning more about gynecologic pathology to consult these standard textbooks.
In my notes, the most helpful current journal references are embedded in the text. Students using these during lecture strongly prefer this. And because the site is constantly being updated, numbered endnotes would be unmanageable. What's available online, and for whom, is always changing. Most public libraries will be happy to help you get an article that you need. Good luck on your own searches, and again, if there is any way in which I can help you, please contact me at scalpel_blade@yahoo.com. No texting or chat messages, please. Ordinary e-mails are welcome. Health and friendship!

| New visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if people like me who call ourselves Christians didn't try to act as good as other good people ." Prayer Request

| If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |
Teaching Pathology
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |
 |
Click here to
see the author prove you can have fun skydiving without being world-class. Click here to see the author's friend, Dr. Ken Savage, do it right. |


 Cytopathology
Cytopathology
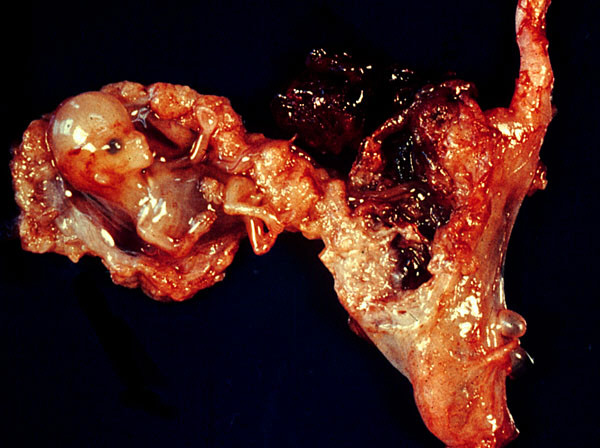 Ectopic pregnancy
Ectopic pregnancy