Ed Friedlander, M.D., Pathologist
scalpel_blade@yahoo.com
No texting or chat messages, please. Ordinary e-mails are welcome.
|
|
 |
 |
 |
 |
|
verify here. |
Cyberfriends: The help you're looking for is probably here.
This website collects no information. If you e-mail me, neither your e-mail address nor any other information will ever be passed on to any third party, unless required by law.
This page was last modified January 1, 2016.
I have no sponsors and do not host paid advertisements. All external links are provided freely to sites that I believe my visitors will find helpful.
Welcome to Ed's Pathology Notes, placed here originally for the convenience of medical students at my school. You need to check the accuracy of any information, from any source, against other credible sources. I cannot diagnose or treat over the web, I cannot comment on the health care you have already received, and these notes cannot substitute for your own doctor's care. I am good at helping people find resources and answers. If you need me, send me an E-mail at scalpel_blade@yahoo.com Your confidentiality is completely respected. No texting or chat messages, please. Ordinary e-mails are welcome.
 I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
I am active in HealthTap,
which provides free medical guidance from your cell phone.
There is also a fee site at
www.afraidtoask.com.
 If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |

|
 |
With one of four large boxes of "Pathguy" replies. |
 I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
I'm still doing my best to answer
everybody.
Sometimes I get backlogged,
sometimes my E-mail crashes, and sometimes my
literature search software crashes. If you've not heard
from me in a week, post me again. I send my most
challenging questions to the medical student pathology
interest group, minus the name, but with your E-mail
where you can receive a reply.
Numbers in {curly braces} are from the magnificent Slice of Life videodisk. No medical student should be without access to this wonderful resource.
 I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
I am presently adding clickable links to
images in these notes. Let me know about good online
sources in addition to these:
 My team:
My team:
pathology.org -- my cyberfriends, great for current news and browsing for the general public
EnjoyPath -- a great resource for everyone, from beginning medical students to pathologists with years of experience
Medmark Pathology -- massive listing of pathology sites
Estimating the Time of Death -- computer program right on a webpage
Pathology Field Guide -- recognizing anatomic lesions, no pictures
Freely have you received, freely give. -- Matthew 10:8. My site receives an enormous amount of traffic, and I'm still handling dozens of requests for information weekly, all as a public service.
Pathology's modern founder, Rudolf Virchow M.D., left a legacy of realism and social conscience for the discipline. I am a mainstream Christian, a man of science, and a proponent of common sense and common kindness. I am an outspoken enemy of all the make-believe and bunk that interfere with peoples' health, reasonable freedom, and happiness. I talk and write straight, and without apology.
Throughout these notes, I am speaking only for myself, and not for any employer, organization, or associate.
Special thanks to my friend and colleague, Charles Wheeler M.D., pathologist and former Kansas City mayor. Thanks also to the real Patch Adams M.D., who wrote me encouragement when we were both beginning our unusual medical careers.
If you're a private individual who's enjoyed this site, and want to say, "Thank you, Ed!", then what I'd like best is a contribution to the Episcopalian home for abandoned, neglected, and abused kids in Nevada:
My home page
More of my notes
My medical students
Especially if you're looking for information on a disease with a name that you know, here are a couple of great places for you to go right now and use Medline, which will allow you to find every relevant current scientific publication. You owe it to yourself to learn to use this invaluable internet resource. Not only will you find some information immediately, but you'll have references to journal articles that you can obtain by interlibrary loan, plus the names of the world's foremost experts and their institutions.
Alternative (complementary) medicine has made real progress since my generally-unfavorable 1983 review. If you are interested in complementary medicine, then I would urge you to visit my new 8Alternative Medicine page. If you are looking for something on complementary medicine, please go first to the American Association of Naturopathic Physicians. And for your enjoyment... here are some of my old pathology exams for medical school undergraduates.
I cannot examine every claim that my correspondents
share with me. Sometimes the independent thinkers
prove to be correct, and paradigms shift as a result.
You also know that extraordinary claims require
extraordinary evidence. When a discovery proves to
square with the observable world, scientists make
reputations by confirming it, and corporations
are soon making profits from it. When a
decades-old claim by a "persecuted genius"
finds no acceptance from mainstream science,
it probably failed some basic experimental tests designed
to eliminate self-deception. If you ask me about
something like this, I will simply invite you to
do some tests yourself, perhaps as a high-school
science project. Who knows? Perhaps
it'll be you who makes the next great discovery!
Our world is full of people who have found peace, fulfillment, and friendship
by suspending their own reasoning and
simply accepting a single authority that seems wise and good.
I've learned that they leave the movements when, and only when, they
discover they have been maliciously deceived.
In the meantime, nothing that I can say or do will
convince such people that I am a decent human being. I no longer
answer my crank mail.
This site is my hobby, and I do not accept donations, though I appreciate those who have offered to help.
During the eighteen years my site has been online, it's proved to be one of the most popular of all internet sites for undergraduate physician and allied-health education. It is so well-known that I'm not worried about borrowers. I never refuse requests from colleagues for permission to adapt or duplicate it for their own courses... and many do. So, fellow-teachers, help yourselves. Don't sell it for a profit, don't use it for a bad purpose, and at some time in your course, mention me as author and William Carey as my institution. Drop me a note about your successes. And special thanks to everyone who's helped and encouraged me, and especially the people at William Carey for making it still possible, and my teaching assistants over the years.
Whatever you're looking for on the web, I hope you find it, here or elsewhere. Health and friendship!
BIBLIOGRAPHY / FURTHER READING
I urge anyone interested in learning more about cancer pathology to consult these standard textbooks.
In my notes, the most helpful current journal references are embedded in the text. Students using these during lecture strongly prefer this. And because the site is constantly being updated, numbered endnotes would be unmanageable. What's available online, and for whom, is always changing. Most public libraries will be happy to help you get an article that you need. Good luck on your own searches, and again, if there is any way in which I can help you, please contact me at scalpel_blade@yahoo.com. No texting or chat messages, please. Ordinary e-mails are welcome. Health and friendship!

![]()
![]()
Define "tumors" and "neoplasms". Tell why they are important. Define "oncology". Tell how tumors are like organs, and how they are different.
Distinguish "benign tumors" and "malignant tumors" by their gross and microscopic appearances and their behaviors. Tell what "well-differentiated" and "poorly differentiated" mean. Tell how benign tumors can cause problems.
Define "cancer", "malignant", and "metastasis". Tell what any cancer will ultimately do to the patient if it is not cured. Recognize the typical appearances of cancers. Distinguish "carcinomas" and "sarcomas".
Tell how and where various cancers tend to metastasize. Describe patterns for invasion and metastasis by various malignant tumors.
List the three most common cancers in men and in women, and the three most common fatal ones.
Given a tumor name, name the cell of origin and describe the behavior. Given the cell of origin (or a hint) and the behavior (or a hint), name the tumor.
Distinguish "grade" and "stage" of a cancer. Tell why these numbers are important.
Recognize, under the microscope, a squamous cell carcinoma, an adenoma, an adenocarcinoma, a tumor of hematologic origin, and a spindle cell sarcoma. Recognize anaplasia, and generally tell benign from malignant tumors.
Critique the following statement, overheard on a cancer ward: "Cancer cells grow faster than normal cells and are not under the body's control. Therefore, the treatment for cancer involves giving anti-mitotic drugs that kill fast-growing cells."
![]() KCUMB Students
KCUMB Students
"Big Robbins" -- Neoplasia
Lectures follow Textbook
QUIZBANK: See next handout
LEARN FIRST
Tumors (neoplasms) may be considered new, useless organs.
Cancers (malignant neoplasms) invade and spread to remote sites (metastasize). The original tumor is called the PRIMARY.
Benign tumors cannot invade or spread to remote sites, but they can cause problems by compressing local structures.
Tumors arise from single cells, and they recapitulate, more or less, the things that cell did in health. The cell of origin gives its name to the tumor.
Benign tumors are usually round like balls. Cancers look like cauliflowers, ulcers, or else simply expand the organ.
Cancers that arise from epithelium are called "carcinomas". Cancers that arise from mesenchyme/mesoderm are called "sarcomas".
Of course, ectoderm is also the source of nervous tissue, but tumors arising here are less common than carcinomas.
Cancers arising from mesoderm can be carcinomas (i.e., adrenals, genitourinary), sarcomas (solid connective tissue and all sorts of muscle), or cells of hematopoietic origin (leukemias, lymphomas).
Both the appearance of the individual cells and the histologic architecture in benign tumors are similar to normal histology. Cells and microscopic architecture in cancers are bizarre. The grade of a cancer is a function of how bizarre the cells look. The higher the grade, the more likely to cancer is to behave aggressively.
The stage of a cancer is how far the clinician knows it has spread.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
One out of about every five persons in the US who die this year will die of tumors (about 500,000 total).
For the foreseeable future, all tumor diagnoses will be made by us anatomic pathologists, using conventional light microscopy as our primary tool.
* DNA microarray technology, while fascinating, is still almost exclusively a research tool. See Am. J. Path. 171: 375, 2007.
* "Tumor"--literally any swelling. Galen distinguished tumors that are:
"natural"--pregnant uterus; think of others
"unnatural"--pus, nodule of healing bone at a fracture site ("callus")
"contrary to nature"--what we now know as neoplasms ("new growths")
The ancient medical writings show an awareness of cancer, and Morgagni remarked that by his era, most physicians were aware that tumors were not treatable except by surgery.
"Oncology" is the study of tumors. In current usage, an oncologist is an internist or surgeon who specializes in the administration of cancer chemotherapy.
In modern usage, a TUMOR/NEOPLASM (the words are exact synonyms) may be thought of as an attempt by the body under some stimulus to make some new sort of organ. It develops in the wrong shape, in the wrong place, and it persists after the initiating stimulus is removed.
Tumors are LIKE organs:
All have parenchyma and stroma.
Cells usually look similar to cells in the organ where the tumor arose.
Cells will continue to perform some of the functions of the parent organ and express most of the same proteins.
Tumors are DIFFERENT from organs:
They don't contribute to the homeostasis of the body.
They usually grow more rapidly than surrounding tissues.
Some benign and all malignant tumors never cease to grow.
"Spontaneous regression" of a cancer (i.e., massive shrinkage or disappearance without adequate therapy to explain it) is much-discussed phenomenon that occasionally happens. More often than not, the cancer comes back after a few months. The phenomenon is fairly well known in CNS lymphomas (Neurology 59: 762, 2002) and melanomas (areas of "partial regression" are often seen in the primary; Am. J. Clin. Path. 124: 37, 2005; it's a good prognostic indicator J. Clin. Path. 61: 297, 2008; one metastasized melanoma in 400 will spontaneously regress Melanoma Res. 18: 279, 2008; also Am. J. Dermpath. 30: 178, 2008); the basis (especially in the latter) is almost certainly an immune attack. If there are metastases, they may or may not also disappear.
Spontaneous remissions of other cancers are less common. There are perhaps fifty reported hepatocellular carcinomas that "self-cured"; how many stayed cured is unknown (Eur. J. Gastro. 20: 804, 2008). Primary melanomas and primary testicular cancers (J. Urol. 182: 2303, 2009) are famous for occasionally vanishing, leaving their metastases behind. Non-small-cell lung cancer sometimes spontaneous regresses completely on its own, but of course comes back (Chest 140: 527, 2011).
A few pediatric cancers, notably neuroblastoma, often self-cure. They all arise from cells that are programmed to die anyway as the child gets older. More about this later.
Testicular carcinomas often present as metastases, with the primary no longer detectable except perhaps as a scar (Am. J. Surg. Path. 30: 858, 2006; J. Urol. 182: 2303, 2009 -- take it anyway as there's likely to be viable cancer).
* You may hear more in the future about the "abscopal" / "distant bystander effect", in which local treatment (radiation or otherwise) results in regression of distant tumor masses "due to immunity". Controversial. See Cancer Treatment Reviews 31: 159, 2005; J. Clin. Path. 62: 647, 2009.
Benign tumors regress by mechanisms that are better-understood. Uterine leiomyomas, being estrogen-dependent, regress at menopause. Hemangiomas undergo thrombosis and self-destruct; especially in children, the "leave it alone" approach is often best (Plast. Recon. Surg. 125: 265, 2010; Plast. Recon. Surg. 127: 1643, 2011).
Most tumors show some derangement of histologic architecture.
Malignant tumors are locally invasive and have metastatic potential.
We have already learned a few essential terms:
Neoplasia: A new, useless organ produced by cells bearing mutations.
Dysplasia: Ugly cells in an epithelium, without invasion. Near-synonyms are "carcinoma in situ", "intraepithelial neoplasia", "incipient neoplasia", "precancer", and (most popular today) "intraepithelial lesion".
Benign: (1) A neoplasm that will compress but not invade the surrounding tissue. (2) Loosely, any non-cancer, non-precancer diagnosis.
A tumor is either BENIGN or MALIGNANT.
Characteristics of BENIGN ("good") tumors:
|
{08800} benign colonic polyp; recapitulates colon
|
![]()
{14165} benign ovarian cystic tumor; it weighed approximately 30 lb
{17488} benign fibroadenoma of breast
Characteristics of MALIGNANT ("bad") tumors
Malignant tumors generally grow more rapidly than benign tumors.
However, no malignant tumor grows as rapidly as an embryo, nor do cancer cells divide nearly as fast as cells in normal bone marrow or intestinal epithelium. Today, anyone who thinks of cancer cells growing "without any control" is guilty of willful ignorance
Cells differ morphologically and functionally from normal cells, and tumor architecture is less organized than that of parent tissue.
Tumor cells are locally invasive; the tumor grows into the surrounding tissue and destroys it.
![]() This feature led Dr. Hippocrates to call such tumors karkinoma after
karkinos, Greek for "crab."
(Cancer is Latin for "crab".)
This feature led Dr. Hippocrates to call such tumors karkinoma after
karkinos, Greek for "crab."
(Cancer is Latin for "crab".)
|
|
![]() Metaphase
Metaphase
Cancer cell in division
Dave Barber MD, KCUMB
The tumor will eventually metastasize, spreading to another site remote from the original tumor (exceptions: basal cell carcinomas of skin, cancers of glial origin).
MALIGNANT TUMOR and CANCER are synonyms.
Benign or malignant, each tumor has a "cell of origin" from its tissue.
Old studies proved that women heterozygous for G6PD variants express only one form in each uterine tumor because of lyonization. And we've long known that plasma cell myeloma produces a monoclonal immunoglobulin product. More about "Nowell's law" soon.
Tumor cells almost always mimic one cell type of some normal organ, usually the one in which the tumor arose.
Cells may continue to elaborate keratin, mucus, hormones, immune globulin, etc. And they may show cross-striations (skeletal muscle cells), microvilli (certain glandular cancers), melanosomes (melanocyte cancer)., etc., etc.
The resemblance will be better or worse depending on whether the tumor is "well-differentiated" or "poorly differentiated."
Much of the day-to-day work of a surgical pathologist is figuring out the cell of origin of poorly-differentiated cancers. The main tools are electron microscopy (now mostly passé) and immunoperoxidase stains ("the brown revolution").
Worth learning now:
These arise anywhere there is a stratified squamous epithelium, either healthy (skin, esophagus, mouth, many others) or metaplastic (endocervix, bronchi).
Look for any (or even all) of the following:
The better these things show, the better-differentiated the tumor! (Benign squamous tumors are uninteresting connective tissue covered with almost-normal-looking stratified squamous epithelium.)
{10085} squamous cell carcinoma
{10088} squamous cell carcinoma, sort-of-good desmosomes
{08977} squamous cell carcinoma, sort-of-good pearls
{09157} squamous cell carcinoma, good desmosomes
{09159} squamous cell carcinoma, electron micrograph,
tonofilaments in the cell on the right
{10987} squamous cell carcinoma, very good pearls
{12596} squamous cell carcinoma, keratin is very pink,
sort-of pearls
{15424} squamous cell carcinoma, good pearls
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
![]() Adenocarcinoma
Adenocarcinoma
Prostate
ERF/KCUMB
![]() Adenocarcinoma
Adenocarcinoma
Prostate
ERF/KCUMB
![]() Adenocarcinoma
Adenocarcinoma
Prostate
ERF/KCUMB
|
|
|
|
|
{00129} adenocarcinoma, apocrine
{08806} adenocarcinoma of colon; low-power
shot shows it arising from the mucosa and pushing toward the
muscularis propria
{08852} adenocarcinoma of the pancreas;
find some odd glands and some signet-ring cells
{08865} prostate adenocarcinoma; some swiss cheese
{08866} prostate adenocarcinoma; some swiss cheese
 |
 |
 |
|
|
LEUKEMIAS AND LYMPHOMAS
Look for cells that resemble blood precursors, not sticking tightly together. (These features distinguish these common cancers from carcinomas and sarcomas.)
{23776} acute leukemia, basophils predominate
|
Immunostains worth learning now:
Benign tumors may cause problems:
The tumor may secrete something in excess (typically a hormone).
The tumor may compress surrounding structures.
{00221} meningioma compressing brain
{01855} craniopharyngioma
A few benign tumors sometimes transform into malignant tumors. Once this happens, they are no longer benign (so, benign tumors never metastasize).
In some syndromes, benign tumors may be multiple.
Malignant tumors in the U.S (American Cancer Society, 2011):
The most common cancers in the U.S. (by occurrence):
Males (in descending order): prostate (240890), lung (115060), colon-rectum (71850)
Females (in descending order): breast (230480), lung (106070), colon-rectum (69360)
The most commonly cancer KILLERS in the U.S.:
Males (in descending order): lung (85600), prostate (33720), colon-rectum (25250)
Females (in descending order): lung (71340), breast (39520), colon-rectum (24130)
NOTE: Worldwide (WHO 2009), the great cancer killers are lung (1.3 million), stomach (803,000), colorectal (639,000), liver (610,000), and breast (519,000). Among men, in descending order: lung, stomach, liver, colorectal, esophagus, and prostate. Among women: Breast, lung, stomach, colorectal, cervix.
NOTE: Worldwide, cancer of the cervix is the great non-obstetrical killer of young women.
NOTE: The other great killer in some of the poor nations is hepatocellular carcinoma, which is primarily a man's tumor (because of hepatitis B carrier status and iron overload).
Thanks to the decline in deaths from atherosclerosis, cancer is now the leading cause of death in U.S. females, and is about tied with atherosclerosis for US males.
What do cancers look like?
You remember that benign tumors are usually round like a ball. (The same can be true of some very tame cancers.)
The Gross appearances of cancers usually fits one of three patterns:
EXOPHYTIC: tumor grows as a lump, often with a cauliflower-like surface ("fungating"; smoother tumors are "polypoid").
(Malignant tumors seldom appear "encapsulated.")
{05801} fibrosarcoma; here and below,
we'll want microscopy for confirmation
{05831} fibrosarcoma
{05834} liposarcoma
{05958} chondrosarcoma
{08437} uterine adenocarcinoma ("cottage cheese
in the uterine cavity")
{08916} uterine adenocarcinoma
{10208} colon adenocarcinoma
{10211} colon adenocarcinoma, in section
{10435} bronchogenic carcinoma
{17511} gastric adenocarcinoma
{11087} squamous cell carcinoma of larynx
ENDOPHYTIC: tumor grows as an ulcer (i.e., the part that was probably protruding from the surface sloughed).
{09810} esophageal carcinoma
{10436} lip cancer
{12169} lip cancer
INFILTRATING: tumor cells invade an organ diffusely without changing its shape.
{01573} brain cancer (glioblastoma)
{01596} same; microscopy
{01599} same; microscopy
Any cancer is likely to exhibit HEMORRHAGE and/or NECROSIS, grossly and microscopically. These result from the cancer cells invading the tumor's own blood vessels.
|
|
|
Microscopic appearance:
Individual cell morphology and tumor architecture may be "well-differentiated" (good prognosis) to "poorly-differentiated" ("anaplastic", bad prognosis).
The malignant-looking cell:
|
|
|
|
|
|
{00132} bizarre mitotic figure
* Better measures of cell division, useful in prognosticating tumors, include immunostaining for PCNA (proliferating cell nuclear antigen) and MIB-1/Ki-67.
There MAY also be microscopic visible INVASION (tumor cells growing into adjacent normal structures where they don't belong), and/or indirect evidence (hemorrhage and/or necrosis; either is important evidence that the tumor in question is malignant).
{10478} squamous cell carcinoma invading; be sure you can recognize the tentacles ("tumor cords") cut in cross section
Usually, the more abnormal a tumor appears under the microscope, the more rapidly it grows and the worse the patient's prognosis.
How will I see malignant tumors invading?
Local infiltration
Invasion of surrounding tissues
For some reason, cartilage, tendon, and elastic tissue almost never get invaded.
{08845} cholangiocarcinoma invading around a nerve ("perineural invasion")
"Intraepithelial spread" is possible and may take the form of single cells ("Paget's disease" of the nipple from an underlying breast cancer, many melanomas) or of DYSPLASIA / CARCINOMA IN SITU, in which an epithelial surface is replaced by a layer of anaplastic cells that has not (yet) penetrated the basement membrane.
Second idea: "Dysplasia is reversible and carcinoma in situ is not." I have been hearing this since I entered medical school without anybody ever explaining why I should believe it. How are you going to tell? Today, some people are managing milder cervical dysplasias "conservatively", we know the likelihood of regression depends on the virus (Ob. Gyn. 113: 18, 2009) and what genes are still working (J. Clin. Path. 64: 303, 2011), but still no one is leaving the high-grade carcinoma-in-situ alone. However, nobody would "just watch" a high-grade intra-epithelial lesion "to see whether it goes away by itself".
Third idea: "Who cares? Call them both INTRAEPITHELIAL ANAPLASIA. Mild, moderate, or severe." This made so much sense that Bethesda decided in the 1990's to call them "intraepithelial neoplasia" instead. Realizing the error, their current term is "intraepithelial lesion."
{08912} carcinoma in situ, endocervix (junction with normal, i.e., the "carcino-columnar junction")
![]() Carcinoma in situ
Carcinoma in situ
Urbana Atlas of Pathology
Metastatic spread:
There are four routes:
(1) Seeding of serosal surfaces (or, in the case of CNS tumors, up and down the neuraxis in the CSF)
(2) Mechanical transplantation (rare, typically iatrogenic; see for example Br. J. Surg. 81: 648, 1994)
(3) Via lymphatics (traditional route for tumors of epithelial origin, i.e., carcinomas)
Tumors spread first to regional lymph nodes, then (because of disruption of directions of lymph flow) to any lymph nodes or organs
{21051} carcinoma in lymphatics (small intestinal
mesentery)
{21052} carcinoma in lymphatics
|
|
|
|
(4) Via blood vessels (traditional route for tumors of mesenchymal origin, i.e., sarcomas, because the tumor cells are in direct contact with blood vessels from the beginning)
Regardless of the route of metastatic spread, certain tumors have unexplained preference for certain metastatic sites.
Why? Even today, there's no clear molecular explanation.
The common sites for metastatic spread for many common cancers include lymph nodes, lung, liver, bone, and brain.
Most cancers won't metastasize to the skeletal muscles, spleen or subcutaneous fat.
Requirements for successful metastatic spread:
"Tumor angiogenesis factor" (more about this momentarily...)
Collagen production by local fibroblasts (if dense, tumor is called "desmoplastic")
Metastatic nodules are called "metastases" or (vulgarly) "mets".
{08443} "liver mets"
{08444} "liver mets"
|
|
|
|
|
|
* There has always been a lot of interest in the basic biology of the metastatic process. It remains an array of tantalizing clues. More on this in your next lecture.
Malignant tumors: Grade and Stage:
The grade and stage of a cancer are determined to offer a prognosis and to determine treatment.
Both grade and stage are usually represented by Roman numerals, the best situation by I, the worst by III, IV, or V depending on the tumor type and determined by rules. Do not confuse grade and stage!
TUMOR GRADE: assigned by the pathologist to reflect the cancer's degree of differentiation. You won't be doing this yourself for your patients, but we will teach you some of the systems.
Grade I: Well-differentiated, cells look like normal organ (benign = Grade 0)
Grade II: Not so well-differentiated
Grade III: Worse than that
Grade IV: Even worse
Grade V: Worst of all (most tumor types are graded I-III or I-IV)
Leave the arcana of grading up to us for now. Rules are constantly changing, and new prognostic factors emerging.
TUMOR STAGE: assigned by the clinician on the basis of all available information on the extent of tumor spread.
Stage I might mean the tumor is smaller than 1 cm diameter, without metastases
Stage II might mean the tumor is larger than 1 cm and/or is symptomatic and/or there are metastases to the regional lymph nodes
Stage III might mean the tumor has infiltrated a non-resectable structure and/or there are distant metastases
Rules for assigning stage are quite elaborate and different for each type of tumor.
Alternative system: TNM
"T" for tumor:
T1 might mean primary tumor is smaller than 1 cm in diameter
T2 might mean primary tumor is larger than 1 cm in diameter
T3 might mean primary tumor is invading something non-resectable
"N" for regional lymph nodes:
N0 would mean no tumor in regional lymph nodes
N1 might mean tumor in a few nearby lymph nodes
N2 might mean many nodes, or some nodes farther downstream, are involved
"M" for metastases:
M0 would mean no distant metastases
M1 would imply distant metastases, etc.
* So the TNM stage for a lung cancer that is invading or encasing the superior vena cava but has metastases only in two nearby lymph nodes might be T3 N1 M0.
Memorizing tumor staging systems is not an appropriate pathology learning objective, and I will not test you on it.
Generally tumors of high GRADE present at high STAGE, while tumors of low GRADE present at low STAGE.
I. To assign a name to a tumor that you have examined, begin by writing the suffix -OMA. Most tumor names end in this way. (Unfortunately, the suffix simply means "swelling", and some non-neoplasms also use the suffix, i.e., GRANULOMA, HEMATOMA, XANTHOMA, traumatic NEUROMA, and "gossypiboma" for a sponge left in after surgery Am. J. For. Med. Path. 33: 54, 2012).
II. If the tumor is MALIGNANT, write the root CARCIN- ("crab") if the tumor is of epithelial origin, or SARC- ("flesh") if the tumor is of mesenchymal origin, before -OMA. If the tumor is BENIGN, do not write anything.
III. Now choose one or more roots to describe the cell of origin.
If the tumor originated in GLANDULAR epithelium, use the root ADENO-. (It probably makes little glands and/or mucin.)
If the tumor originated in SQUAMOUS or UROTHELIUM (formerly called "transitional epithelium"), is BENIGN, and protrudes above the epithelial surface, use the root PAPILLO-. If it meets the first two criteria but does not protrude, the pathologist knows the name but you don't need to just now.
If the tumor originated in NON-GLANDULAR EPITHELIUM and is MALIGNANT, name it for the cell of origin.
If the tumor originated from a NON-EPITHELIAL cell, look for a root in the following list. (We do not consider endothelium and mesothelium to be epithelium for this purpose.)
There are a few epithelial roots you will have to learn. For example:
CHORIO-: placenta
PHEOCHROMOCYTO-: adrenal medulla and similar tissue
If the neoplastic cell types are MIXED, use a compound, for example, fibroadenoma.
| Some tumors arise in "totipotential cells" and contain a variety of different mature and/or immature tissues from different germ layers, and these are given names with the root TERATO- ("monster"). |
 |
|
|
IV. You can add adjectives as appropriate.
papillary
well-differentiated
keratinizing
moderately well-differentiated
mucin-producing
poorly differentiated
follicular
pleomorphic
signet-ring cell
cystic (CYSTO-)
scirrhus
desmoplastic
medullary
comedo-
tall cell
clear cell
serrated
V. A handful of tumors that are thoroughly malignant have "benign" names. You will just have to learn these.
VI. A HAMARTOMA is "not a tumor, but is a developmental anomaly" (?) that contains the same tissues as the organ in which it is found, but in the wrong proportions.
A CHORISTOMA ("ectopia") is a mass of normal tissue in an abnormal location.
A tumor that ends in BLASTOMA is composed of cells that resemble those seen in a developing organ. Most blastomas are malignant (but it depends on the site).
A few tumors of uncertain histogenesis are named EPONYMOUSLY: Ewing's sarcoma, Hodgkin's disease, Pindborg tumor, Wilms' tumor, Enzinger's sarcoma.
A POLYP describes a gross appearance rather than what's actually happening. It might be a cancer, a benign tumor, a hamartoma, a choristoma, or a hyperplasia such as a singer's vocal cord polyp. The term won't appear without a clarifier on a pathology report.

| New visitors to www.pathguy.com reset Jan. 30, 2005: |
Ed says, "This world would be a sorry place if people like me who call ourselves Christians didn't try to act as good as other good people ." Prayer Request

| If you have a Second Life account, please visit my teammates and me at the Medical Examiner's office. |
Teaching Pathology
 Ed's Pathology Review for USMLE I
Ed's Pathology Review for USMLE I
![]()
![]()
 | Pathological Chess |
 |
Taser Video 83.4 MB 7:26 min |
 |
Click here to
see the author prove you can have fun skydiving without being world-class. Click here to see the author's friend, Dr. Ken Savage, do it right. |


 Neoplasia
Neoplasia
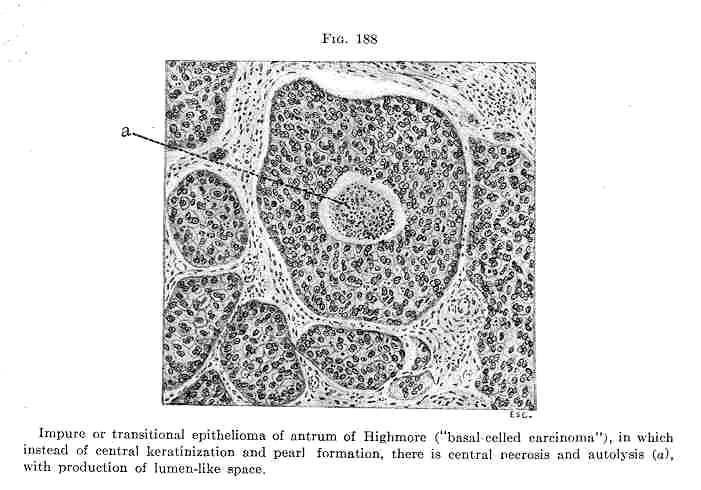 Carcinoma with necrosis
Carcinoma with necrosis